The term 'DIABESITY' is used to denote the combination of diabetes and obesity which is rapidly emerging as a major public health concern across India (100 million diabetics & 250 million obese people). Modern stressful lifestyle with low physical activity and high consumption of bad foods seems to be the underlying cause.
Dr. T. Rama Prasad
This may be called the new "Cursed Duet" of the day. This has come to stay, as the bad lifestyle evolved over the past half-a-century can't be reversed.
Globally, the economic loss due to obesity is predicted to reach $3 trillion annually by 2030. India's GDM (pregnancy diabetes) is 3.5 times more than Western countries; about 1 in 5 pregnant women have GDM ((ICMR - STRIDE study).
Obesity and Diabetes are complex chronic diseases which are drivers of a plethora of other diseases. They are not just about 'diet & exercise' which are closely associated with them.
An injection a week keeps the "Obesity & Diabetes" away !!!
Will "An apple a day keep the doctor away" ???
GLP or no-GLP, the 'Cursed Duet' will take its toll.
The simple 1-h PG test and WHR may predict or diagnose diabetes and obesity.
The new WEIGHT LOSS & DIABETES drugs:
Per month, the drugs may cost Rs. 14,000 to 27,000, as in August 2025. As in December 2025, with the introduction of OZEMPIC (semaglutide) in the Indian market, the cost has come down to Rs. 8,800 per month (0.25 mg 4 times a month -- around half the price of other similar drugs).
An ad without mentioning the drug
Reacting to the recent ads, the DRUG INDUSTRY is warned in March 2026 by the India's DRUG REGULATOR against public advertisements or campaigns to promote the new WEIGHT-LOSS DRUGS directly or indirectly (in the guise of 'disease awareness' even with 'protective disclaimers'). It's not like "An injection a week keeps the weight away." Long term side effects are yet to be documented. For more on this subject, click on : https://drtramaprasad.blogspot.com/2017/04/diabetes_29.html -- Dr. T. Rama Prasad, Perundurai, India
Ozempic is now (December 2025) directly imported from Denmark, and is available in India as 0.25 mg, 0.5 mg and 1 mg strengths in 'Flex Touch Pen' - an easy-to-use, once-weekly injection device, at Rs 2,200 per week of a dose of 0.25 mg. Danish Pharma major Novo Nordisk produces two brands of semaglutide -- Ozempic and Wegovy. Wegovy, at double the price of Ozempic, is already available in India since several months.
Overweight and obesity are conditionsofabnormalfataccumulationthatincrease healthrisks,primarilydefinedbyBodyMassIndex(BMI): overweight is a BMI of 25.0–29.9, while obesity is a BMI of 30.0 or higher, with obesity further classified into classes (Class 1, 2, 3) based on BMI ranges (30-34.9, 35-39.9, 40+). Less than 18.5 is considered as underweight. For more details about this, go to :
BIG Pharma's BIG Money
MOUNJARO (tirzepatide of Eli Lilly company -- pre-filled device, KwikPen-- monthly cost is above Rs. 14,000) is India's No.1 pharma brand with recorded sales of as much as Rs. 100 crore in the month of October 2025. WEGOVY (semaglutide of Novo Nordisk company --monthly cost is above Rs. 17,000) sales were of Rs. 10 crore.
Mounjaro has become the top selling drug in India -- Rs. 100 crore in October 2025. This is just for one product of the latest "weight loss drugs." The reasons for this boost are : 1. high cost of the drug, ironically, 2. many millionaires are obese and diabetics. 3. aggressive marketing through "BIG" prescribers who may not necessarily be sure of the outcome. With the introduction, in December 2025, of Ozempic, at half the price, the sales of Wegovy and Mounjaro may come down drastically. In India, the patent on SEMAGLUTIDE (Ozempic & Wegovy) expires in March 2026 following which several companies would make this drug much cheaper ( Rs 750 to Rs 2,000 -- a drop of 50 - 90 %). The steep drop in the price may promote misuse and overuse of these drugs.
The "BIG PHARMA" knows that the cheapest drug for "Obesity & Diabetes" is "Diet & Exercise & Good lifestyle" which cannot be taken by the 'modern folk' addicted to bad things. So, to grow BIGGER, the "BIG PHARMA" launched the weekly injection against "Obesity & Diabetes" in March 2025 in India priced at Rs. 4,375 -- Mounjaro (Tirzepatide 5 mg) -- to be taken every week. Though the price seems to be high, it is claimed to save billions of rupees and millions of lives by preventing complications due to obesity and diabetes. Thanks to the "BIG PHARMA."
Analysts expect that the world market for obesity therapy drugs could touch $100 billion by the end of this decade.
SEMAGLUTIDE (Wegovy / Ozempic) and TIRZEPATIDE (Mounjaro) -- injectable GLP-1 drugs for Type 2 diabetes and obesity -- are approved by the FDA of USA and are available in India in 2025. Poviztra (semaglutide) will be available in India in 2026. GLP-1 means 'Glucagon-like peptide-1' which is a hormone involved in regulating blood sugar levels and appetite. These drugs activate the GLP-1 receptors in the body. A study ( published on June 10, 2025 in the journal OBESITY ) found that these 'weight-loss' drugs didn't have the expected impact in real liife situations as many people discontinued treatment or used lower doses for various reasons.
Obesity and 'Type 2 diabetes' seem to have grown more after the arrival of COVID. Old disorders. New connections. New drugs. New buzzwords like OZEMPIC weekly injections, MOUNJARO weekly injections and ORFORGLIPRON daily tablets. They all may reduce both OBESITY and DIABETES. Two birds in one shot !! It is documented that they may also reduce some risks due to problems related to heart (SOUL trial & STEP-HFpEF trials), blood vessels, kidney and eye (UKPDS & DCCT studies) which are common complications to both obesity and diabetes. Three or even more birds in one shot !!!
Hence, the number of "INFLUENCERS", both inside and outside the profession is growing very fast. The rapid expansion of the use of these drugs raised concers about misuse and overuse. ."SLIM CLINICS" were found to be using these drugs unauthorisedly. Just one brand of the drug was sold to the tune of Rs 100 crore in October 2025. India's drug regulator warned against unauthorised use and misleading ads for marketing.
These drugs of 'GLP-1 group' for patients with diabetes are now approved for obese individuals without diabetes as well for reducing weight.
Wonderful, but not the solution
The weight loss is wonderful and dramatic -- up to 20kg. But, they are not effective without dieting and. exercise. These expensive new drugs -- GLP-1 receptor analogues, twin analogues, dual, triple and quadruple analogues -- may not be a sustainable replacement for the present advisories.
if found to be effective and safe in the long run, and get the necessary approvals, may replace all the present day drugs globally for these two huge chronic disorders. But, notwithstanding the multiple benefits, many are hesitant to use them because of the prick of the needle, high cost, side effects -- known and unknown, etc.
SIDE EFFECTS
Overall, these new drugs are now considered safe. However, severe stomach-related side effects, muscle loss and some eye problems (macular edema arisinng from vascular leakage, tempoorary worsening of diabetic retinopathy due to rapid reduction of HbA1c - SUSTAIN-6 trial). were reported. Patients with pancreatitis and medullary thyroid carcinoma should avoid these drugs. A new study presented at the American Academy of Orthopaedic Surgeons 2026 suggests weight-loss drugs may increase the risk of fractures due to osteoporosis and gout.
Many 'weight-loss' drugs were introduced during the past half-a-century, but most of them had not been in use due to safety issues and side effects. So, dear reader, consult a doctor before having a shot or popping a pill.
“Science is always wrong. It never solves a problem without creating ten more.” -- George Bernard Shaw
Eli Lilly company is poised to sell ORFORGLIPRON tablets instead of the injections from 2026. The tablet is likely to be a game-changer in obesity & diabetes, with an expected market worth of $50 billion by 2030. So, we shall go from "an injection a week" to "a pill a day."
If you can wait for a longer time, there is the possibility that the obesity problem may be solved witth just one (gene therapy) injection !!! There is an experimental GENE THERAPY. The US biotech company FRACTILE HEALTH is developing REJUVA, a therapy designed to help the body produce more of its own GLP-1 hormone which regulates appetite and blood sugar. Though early animal studies showed positive results, human trials are yet to be made. It's a long way. If successful, we need not use the expensive 'GLP-1 drugs' lifelong with unknown long-term side effects.
"New & Expensive" is always welcomed by the wealthy. For example, Hollywood celebrities and Bollywood stars are already using the new "NAD+" injections (Rs.50,000 per dose) to look younger, feel energetic and live longer. 'NAD+' is 'nicotinamide adenine dinucleotide' , an antioxidant coenzyme, in the bioactive form of vitamin B3.
PEPTIDES
Peptides are short chains of amino acids, the basic building blocks of proteins in the body, that regulate hormones, metabolism, immune. responses and reduce inflammation. In therapy, these peptides are used to mimic the body's natural signals and send targeted instructions to certain cells. They are generally better tolerated than some conventional drugs. Some best known and currently popular peptides are in the weight reducing GLP-1 class of drugs (semaglutide, tirzepatide, etc). But in the gray market, many unproven and unapproved peptides are available -- BPC-157, and TB-500 for healing injuries; epitalon for sleep disorders; retatrutide for weight loss; and some others for anything from stomach problems to mind disorders. Many of them come from China, and the US imported more than $300 million in the first nine months of 2025. People are using them as 'biobackers', while the FDA of USA has warned that many peptides pose 'serious safety risks'. However, more than 80 peptide-based drugs are currently being studied, and many of hem are already being used in wellness, fitness and anti-ageing centres, as peptides are promoted as a 'targeted and advanced' way to improve health, appearance and performance. The safety issue remains unknown.
GLP-1
"The glucagon-like peptide-1 (GLP-1) receptor, known as GLP-1R, is a vital component of the G protein-coupled receptor (GPCR) family and is found primarily on the surfaces of various cell types within the human body. This receptor specifically interacts with GLP-1, a key hormone that plays an integral role in regulating blood glucose levels, lipid metabolism, and several other crucial biological functions. ... This receptor and its agonists hold significant therapeutic potential, reshaping the treatment approaches for multiple diseases, including diabetes, cardiovascular disorders, and neurodegenerative diseases.5,6,7GLP-1 is a peptide produced by the cleavage of proglucagon, mainly synthesized in the intestinal mucosal L-cells, pancreatic islet α-cells, and neurons in the nucleus of the solitary tract.3,4GLP-1RAs mimic the action of endogenous GLP-1, activating GLP-1R, thereby enhancing insulin secretion, inhibiting glucagon release, delaying gastric emptying, and reducing food intake through central appetite suppression.8,9,10These mechanisms make GLP-1RAs powerful tools for controlling blood glucose and improving metabolic syndrome.The extensive benefits of using GLP-1RAs in treating a broad spectrum of diseases, such as obesity, cardiovascular diseases, non-alcoholic fatty liver disease (NAFLD), neurodegenerative diseases, musculoskeletal inflammation, and various forms of cancer are documented. " Semaglutide has been approved for metabolic dysfunction-associated steototic liver disease, associated with weight gain and cardio-metabolic disorder.
GLP-1 and the WHO
The World Health Organization (WHO) had added, in May 2025, GLP-1 class of drugs (semaglutide, dulaglutide, liraglutide, and tirzepatide) to the 'Model Lists of Essential Medicines (EML) for treating 'Type 2 diabetics, especially those who also have obesity, cardiovascular, or chronic kidney disease. There are more than 800 million people with diabetes and more than one billion with obesity, world wide in 2022. These costly drugs would be out of the reach to most of these people even if the prices come down to some extent. The WHO's approval may make these very expensive drugs a bit cheaper and more easily available to the public. Of course, some may say that some vested commercial interests might have influenced the 'conservative' organization to put these drugs on the EML, just as they said when the WHO declared Swineflu as a pandemic in those days, and in the COVID times about some emergency approvals. ( https://drtramaprasad.blogspot.com/2017/03/medical-literature.html ) ( https://drtramaprasad.blogspot.com/2017/04/hydroxychloroquine-hcq-and-coronavirus_29.html
).
The WHO went a step further on December 1, 2025, by releasing "The WHO guidelines" on the use of the GLP-1 class of 'weight loss' drugs, implying a recommendation, conditionally though. One of the condition is that dieting and exercise must be continued alongside the drugs. Is the WHO's backing is premature and hasty, in view of the lack of evidence over the safety and efficacy in the long term, and the present high cost which is out of reach for most of the people ?
Some approved GLP-1 (nonpeptide glucagon-like peptide- 1 receptor agonists) medications: Ozempic / Wegovy / Poviztra (Semaglutide Injection) - - https://www.healthline.com/health/drugs/ozempic#_noHeaderPrefixedContentRybelsus - (Semaglutide tablet), Mounjaro (Tirzepatide), Trulicity (Dulaglutide), Victoza / SAxenda (Liraglutide), BydureonBCise / Byetta (Exenatide). Orlistat, Naltrexone-bupropion, and Phenteramine-topiramate are some more of the available medicationns. There are some natural supplements to increase GLP-1 : Berberine, Curcumin, Ginseng, etc.
The following 5 items are the injectable GLP-1 receptor agonists available in India as of October 2025. The first three are approved only for DIABETES, not for the combination of Obesity & Diabetes. All are 'weekly injections except Liraglutide which is given daily.
Drug Name (Brand) - Active Ingredient - Manufacturer - Dosing Frequency - Primary Indications and Notes.
1. Trulicity - Dulaglutide - Eli Lilly - Once weekly - Type 2 diabetes - Holds the largest market share (~78% in 2024); suitable for adults and children aged 10+.
2. Victoza - Liraglutide - Novo Nordisk - Once daily - Type 2 diabetes; cardiovascular risk reductionEstablished option; biosimilars (e.g., from Biocon) approved in 2025 for broader access.
3. Bydureon (Byetta) - Exenatide extended-release - AstraZeneca - Once weeklyType 2 diabetesLess commonly mentioned but available as a standard GLP-1 option.
4. Wegovy & Poviztra - Semaglutide - Novo Nordisk - Once weekly - Type 2 diabetes & obesity; cardiovascular benefits; Widely used off-label for weight loss; imported versions available prior to full approval.
5. Mounjaro - Tirzepatide (dual GLP-1/GIP agonist) - Once weekly - Type 2 diabetes, chronic weight management14,000–17,500 (for starter doses) - Eli Lilly; Officially launched in March 2025; priced at ₹3,500 (2.5 mg vial) and ₹4,375 (5 mg vial), with higher doses more expensive. Available in select pharmacies on prescription.
6. Ozempic (imported) - Semaglutide - Once weeklyType 2 diabetes & obesity ; 20,000–80,000+ earlier, Rs. 8,800 per month sinceDecember 2025; Novo Nordisk; Not officially launched (patent expires 2026); Available via named-patient import programs, often from overseas sources. Marketing in India since December 2025. Biosimilars expected post-2026 under PLI scheme.
"Published on:
United States’ pharmaceutical giant Eli Lilly has launched its weight-loss and diabetes drug, Mounjaro, in India. Known chemically as tirzepatide, the once-weekly injectable medication arrives amid soaring global demand and rising concern over obesity-related complications in the country. However, the price point may still make it out of reach for most Indian patients. Mounjaro is priced at Rs 3,500 for a 2.5 mg vial and Rs 4,375 for a 5 mg vial, translating to Rs 17,500 per month for a patient on a 5 mg weekly dose — raising affordability questions in India’s cost-sensitive healthcare market. The prescription-only weekly injectable drug is designed primarily for people with type 2 diabetes or those with obesity and related health issues like hypertension or heart disease."
October 9, 2025
It is surprising to know that MOUNJARO (tirzepatide of Eli Lilly company -- pre-filled device, KwikPen-- monthly cost is above Rs. 14,000) is now India's No.1 pharma brand with recorded sales of as much as Rs. 100 crore in the month of October 2025. WEGOVY (semaglutide of Novo Nordisk company --monthly cost is above Rs. 17,000) sales were of Rs. 10 crore.
The promotion of these expensive drugs is so good that shortage of these drugs is reported in some "rich" countries (The Lancet, Aug / Sept, 2025)
It may be interesting to know how companies struggle to make new drugs and market them. Of late, there has been a growing suspicion about the veracity of some of the rolled out statistics and the validity of conclusions of some research studies. Read my writing titled "MEDICAL LITERATURE" Go tohttps://drtramaprasad.blogspot.com/2017/03/medical-literature.htmlto know the unknown ! -- read it, it's only a click away. You may be surprised.
Rebekah Carl injects herself with her weekly dose of Wegovy in New Columbia, Pennsylvania, U.S., November 13, 2023.
LOSS REGAINED
Some are expressing the concern of weight gain after stopping 'anti-obesity drugs'. A paper "Trajectory of the body weight after drug diiscontinuation in the treatment of anti-obesity medications" was published in BMC Medicine(July 2025). The review indicated that weight regain begins about eight weeks after stopping the drugs, but that at 52 weeks they weighed less than they did before starting the medication. As the benefits go beyond weight loss, the expensive drugs may be considered as a worthwhile investment.
FUTURE DIABETICS
1-h PG test: Take 75 grams of DEXTROSE (glucose) powder in 300 ml of water by mouth. Get blood glucose estimated after one hour. If it is between 155 mg and 209 mg, one may become a diabetic in future. For more information on this test, go to the subheading "OLD is GOLD" which is a little below.
WDNK
"Obesity and Diabetes are not just about EATING and EXERCISING. And, the treatment is not a ONE-SIZE-FITS-ALL solution. The answer to many questions about these disorders is still "WDNK (We Do Not Know). Some researchers are of the view that it is the excessive consumption of processed and semi-processed packaged foods that is to be blamed (not rice and chappathi) for the increse in the cases of obesity and diabetes, in recent times."
'Frequent small quantities of food' (5 times) had been the advice for diabetics. Now, they say that '3 good meals at 9 am, 1 pm & 8 pm' is better (The Hindu's Wellness Webinar on Nov 13, 2025 -- The Hindu of November 14, 2025). A conundrum !
-- T. Rama Prasad
Are there any type 2 diabetes medicines that can help people lose weight and lower their blood sugar? Are there side effects?
Read further down below the answer from M. Regina Castro, M.D.
Oddly, the Central Board of Secondary Education (CBSE) , not the health authorities, took the initiative to prevent 'obesity and diabetes' in school children. The CBSE has directed its affiliated schools to display "SUGAR BOARDS" to make children aware that excessive consumption of sugar may make them prone to diabetes and obesity.
In recent decades, there has been a significant increase of Type 2 diabetes and obesity in children which could mostly be due to excessive consumption of sugary snacks, sweet beverages, 'energy & health drinks' and a myriad of processed foods, which are often readily available in school environments. Several studies indicate that children have been taking as much as around 15 % of their calories in the form of sugar. Only 5 % is recommended.
The initiative of the CBSE is highly commendable, but it's like reforming a criminal while serving a prison sentence. The children are already spoiled (and will continue to be spoiled) by their parents by addicting them to unhealthy food stuff. Can the CBSE go to their homes and do something ? Parents should be targeted to develop good food habits which they can pass on to their children.
SEDENTARY LIFESTYLES and UNHEALTHY EATING HABITS have been the cause for the increased obesity and diabetes in recent times.
Studies show that adding sugar to any food (including the milk given to infants in bottles / cups) for babies or small children predisposes them to having a sweet tooth. They start preferring sweet things, which is harmful, in their diets throughout their lives. The World Health Organization (WHO) advises against added sugar for infants due to potential long-term health issues like diabetes and other chronic diseases. Go to my 'Scribbling' titled "FOOD, EXERCISE & SLEEP" -- https://drtramaprasad.blogspot.com/2017/04/food-exercise-and-sleep_25.html
OBESITY
The Prime Minister of India, in his monthly radio address Mann Ki Baat'', in February 2025, cautioned against the rising obesity rates in India, particularly among children. Perhaps, the increase is a reflection of prosperity and modernity in lifestyle !!! According to the National Family Health Survey (NFHS-5 , 2019-21, India), 24% of aged 15 - 49 are obese (21% in 2015 - 16). The World Obesity Federation said (2026) that more than 200 million children globally, and 41 million children in India are over-weight.
The study published in the Nature Scientific Journal (2026) by the Health Systems Transformation Platform showed that around half of the Indian population have ABDOMINAL OBESITY due to long hours in sedentary jobs, increased motorised transport, and the widespread consumption of processed foods. The morbidity is seen more in wealthier urban people.
September, 2025: The latest (2025) report of the UNICEF says that, globally, the dominant form of malnutrition is OBESITY among school-age children and adolescents due to unhealthy foods including Ultra Processed Foods (UPFs) and beverages. It mentioned : "In pursuit ofprofit, the industry leverages vast financial resources and deep political influence to resist policies aimed at creating healthier, more equitable food environments."
(1) In general, having a WAIST CIRCUMFERENCE of less than half of the HEIGHT of an individual is healthy. The WAIST / HEIGHT ratio (WHtR) of 0.4 to 0.49 is healthy; 0.5 to 0.59 indicates increased risk; 0.6 or more means high risk. This measurement may be made as a routine check-up for the patients, or even by people at home to know their 'fat status'. It requires only a measuring tape.
(2) And, If you were never tested for diabetes, drink a solution of 75 grams of Dextrose (Glucose) powder in 300 ml of water on empty stomach in the morning and test the blood sugar after one hour. Show the result to your local doctor.
Obesity is a major public health problem worldwide which could not be brought down in spite of a tremendous build up of knowledge and its application. The humongous variety and the huge growth of the remedies to lose weight is a testimony to their failure ! Obesity is being increasingly recognised as a risk factor for becoming a diabetic or a victim for many other diseases including cardio-vascular diseases and even cancer Around a billion people may be having excessive weight in the world. Obesity is a chronic disease influenced by genetics, lifestyle and environmental factors.
Interestingly, some recently introduced 'type2 diabetes medicines' (GLP-1 receptor agonists) like SEMAGLUTIDE (Wegovy / Ozempic) and TIRZEPATIDE (Mounjaro) are being used to reduce excessive body weight even in non-diabeticsfor indefinite periods of time. They are very expensive (around 1,000 dollars per dose in America and around Rs.4,000 in India) and to be administered by injection, once a week. Patients with pancreatitis may not be given these drugs. ORPHORGLIPRON is another new drug which can be given as a daily pill and which is said to be as effective as the above injectables to control obesity and diabetes. It may be in the market by 2026.
Apart from these 'type2 diabetes medicines(GLP-1 receptor agonists)', there are some other drugs known to reduce excessive body weight -- Benzphetamine, Bupropion, Naltrexone, Liraglutide, Oristat, Phendimetrazine, Phentermine, Topiramate, etc. Obesity is a very complex phenomenon, and most of the non-pharmaceutical and pharmaceutical measures didn't stand the test of time.
FATTY HAPPY MAN
The 'obesity drugs' market is expected to cross $100 billion in the next decade ! They would definitely reduce the weight in the pocket !!! What's WRONG ? And what's RIGHT ?
The buzz around the expensive injectable weight-reducing anti-diabetic drugs has got louder with the announcement that TIRZEPATIDE (Mounjaro) and SEMAGLUTIDE (WEGOVY / OZEMPIC) injections will be available in the Indian market by 2025 / 26. The usual dose is one injection every week. Semaglutide is also available as tablets for weight reduction. One tablet a day of ORFORGLIPRON may become very popular. And there are other brands like Liraglutide, Orliistat, etc.
It makes good business sense for the 'pharma-medical' industry to amplify the buzz as India has eight crores of obese people, including one crore in the age group of 5 to 19 years. And also because India is the 'Diabetes Capital' of the world, having more than 20 crores of diabetics. Let alone the prohibitive cost of the injections (the cost would come down with increased usage), would it be WRONG to think that they also won't stand the test of time ?
In the US, around 60% of the patients stopped taking these 'injectable weight-loss drugs' after taking for one year (Journal of Managed Care and Specialty Pharmacy'). The rapid loss of weight is so much in some people that they faced the questions : "Had you been very ill for some time ? How are you now ?" The emaciated appearance called for "SKINVIVE and BOTOX" injections to fill the spaces left by 'fat' !!! Some of them preferred to be round "potatoes" than "bitter gourds" with all the wrinkles and furrows !!!
FATTY HAPPY MAN is the one who sells all these drugs and laughs his way to the bank !!!
FATTY LEAN MAN !!! .
High fat means high cholesterol; high cholesterol means high heart attacks. Right or wrong ? Lean body means low fat; low fat means no heart attacks. Right or wrong ?
FATTY LEAN PERSON !!! How can a lean-looking person be fatty ? In recent years, it is found that some of the people who look normal are loaded with a lot of fat inside their chests and abdomens which makes them vulnerable to metabolic diseases. We used to assess the fat content of a person by just looking at him / her.
Then came the 'Body Mass Index (BMI)' as a standard to estimate the fattiness (mass) of the body (calculated by dividing the weight in kilograms by the height in metres squared -- for a weight of 70 kg and a height of 170 cm, the BMI would be 24.22 (less than 18.5 is considered as underweight, 18.5 to 24.9 is normal, then up to 29.9 is overweight, then up to 34.9 is obesity class I, then up to 39.9 is obesity class II, then over 40 is obesity class III).
It should be noted that body fatness (which is generally equated to bad cholesterol levels) is just one of the various factors that determine the overall health. In fact, certain amount of cholesterol is necessary for maintaining good health. Maintenance of normal body functions is a highly complex one which involves trillions of cells functioning in sync. One disruption may lead to a cascading effect of a disaster.
BMI, WC, WHR, WHtR, BRI, BCA
For about half-a-century, BMI alone has been recommended as the measure to characterise obesity-related morbidity and risk of death due to cardio-metabolic health complications such as type 2 diabetes, high bad cholesterol and cardio-vascular diseases. In recent years, it has come to the knowledge that BMI alone can't give an idea of the fat inside the body (visceral fat), and that a simple measurement of "Waist Circumference (WC)" gives a better assessment.
Until recently, a person, apparently looking physically normal with normal BMI, normal height and weight, normal lifestyle and doing normal work was considered not to have a risk associated with excessive weight, bad cholesterol, diabetes, high blood pressure, heart diseases, etc. as he was supposed not to have excessive fat. Today, it's supposed to be a WRONG assumption, as he may be having a lot of VISCERAL FAT inside his chest and abdomen which can't be assessed by BMI test.
A person of “normal” weight and “normal” BMI may have a lot of VISCERAL FAT (of large organs inside the body), around the heart, lungs, liver, pancreas, etc. !!! And they are at the risk of developing diabetes, cardiovascular disease and ‘metabolic syndrome’.
The RIGHT assumption now is that measurement of "Waist Circumference" gives a better indication than BMI about 'visceral fat load' and the attendant metabolic and cardio-vascular diseases. As such, a set of new measurements to quantify the VISCERAL FAT are coming into vogue which are recommended to be used in addition to BMI.
‘Waist Circumference (WC)’ measurement at the level of umbilicus may give an idea of visceral fat deposition better than the BMI (below 90 cm / 35.4 inches for men and below 80 cm / 31.4 inches for women is normal). The 'Waist to Hip Ratio (WHR)' parameter (below 0.9 for men and below 0.85, and more than 1 is linked to increased risk of heart disease) may be a better option. These two tests, as indicators of good health, require just a measuring tape to do. A couple of other similar tests may give more information -- 'Body Roundness Index (BRI)'to assess abdominal fat content (below 4.5 is normal, above 6.91 is high); 'Body Composition Analysis (BCA)' test gives the percentage of fat (10 to 30 % is normal) , bone and muscle in the body. These two tests can be done by simple machines. Will all this be a WRONG assessment of the risk after sometime !!!
"The National Heart, Lung and Blood Institute (NHLBI), International Diabetes Federation (IDF), and American Heart Institute (AHI) consider only waist measurement. The NHLBI and AHI define a healthy waist size as: 35 inches or less for women. 40 inches or less for men.19 Jul 2024 " Can these measurements be RIGHT for Indians ?
"WAIST to HEIGHT Ratio (WHtR) : In general, having a WAIST CIRCUMFERENCE of less than half of the HEIGHT of an individual is healthy. This may be taken as a 'VITAL SIGN' in clinical practice.
WHtR of 0.4 to 0.49 is healthy; 0.5 to 0.59 indicates increased risk; 0.6 or more means high risk. This measurement may be made as a routine check-up for the patients, or even by people at home to know their 'fat status'. It requires only a measuring tape." -- T. Rama Prasad
INDIAN POTBELLY
South Asians, particularly Indians, tend to accumulate excessive visceral fat. It may start while still in the wombs of malnourished Indian mothers. Excess fat gets deposited, especially in the liver and pancreas. Fat metabolism seems to play as important a role as carbohydrate metabolism. Excess fat in the liver leads to insulin resistance. A fat-loaded pancreas produces less insulin. Curiously, some babies born in India are found to be small in size though they have more fat than a normal proportion --- "Thin Fat Indian Child." When they grow up, they may become TOFIs (Thin Outside and Fat Inside) !!! Some attribute the "Thin-fatty phenomenon" to a "Thrifty Gene" evolved during famines in the past, to build up reserves in the form of visceral fat. If it is genetic, is it modifiable ?
One may say, citing the mythological figures in the epics, that potbelly is a racial characteristic and that efforts to melt it would be an exercise in futility. RIGHT or WRONG ? "Potbelly sculptures' have been associated with FAT GOD of Mesoamerican mythology. Mahabali, Buddha, Kubera, Ganesha and others are visualised as potbellied deities.
Obesity is a major public health problem worldwide which could not be brought down in spite of a tremendous build up of knowledge and its application. What's WRONG ? Can the new drug TIRZEPATIDE set it RIGHT ? This drug under the brand name MOUNJARO of Eli Lilly company costs around 1,000 US dollars per fill. It is expected to be available in the Indian market by 2025. The 'obesity drugs' market is expected to cross $100 billion in the next decade ! They would definitely reduce the weight in the pocket !!!
There are some other drugs known to reduce excessive body weight -- Benzphetamine, Bupropion, Naltrexone, Liraglutide, Oristat, Phendimetrazine, Phentermine, Topiramate, etc. Obesity is a very complex phenomenon, and most of the non-pharmaceutical and pharmaceutical measures didn't stand the test of time.
Interestingly, some recently introduced 'type2 diabetes medicines' (GLP-1 receptor agonists) like SEMAGLUTIDE (Wegovy / Ozempic) and TIRZEPATIDE (Mounjaro) are being used to reduce excessive body weight even in non-diabetics.
--------- India had 64.5 million diabetics in 2015 compared to 11.9 million in 1980 (study by The Lancet released in 2016) and 101 million (ICMR-INDIAB study) in 2020s. And, over 200 million in 2022, according to data published in The Lancet of November 2024. Nearly half of them were women. And, there are 136 million people with 'pre-diabetes' in India now. A recent (2023) ICMR-INDIAB study published in The Lancet found that 11.4% of Indians had diabetes while 35.5% were hypertensive, 39.5% had abdominal obesity and 32.1%had hypertriglyceridemia.
---------- In Tamil Nadu, 10% of the adults in rural areas, 15% in urban areas and 25% in Chennai city are diabetics. And, double this number are 'pre-diabetics'.
--------- It is obvious that the alarming difference in the figures is due to 'BAD LIFESTYLE' -- insufficient exercise, excessive consumption of 'bad' foods, etc. -- read about them under the heading 'Food, exercise & sleep' on this blog. Most of the "fashion foods" of the day which are considered as "normal" by the "modern folk" contain excessive amounts of the deadly "FSS (fat, sugar & salt) ... processed, semi-processed and ultra-processed foods, sweetened soft drinks, colas, pizzas, burgers, noodles, chips, etc.
-- Dr. T. Rama Prasad
"Look, I am human. It's hard to be fair sometimes. We don't always feel the right thing, do the right thing." -- Stephenie Meyer
In my experience of over half-a-century in medical profession, not many diabetics strictly followed diet or life-style advice. That's because they are 'HUMANS' as in the quote above ! It may be obvious that humans can't kill their tastes for the rest of their lives !
"If you were never tested for diabetes, drink a solution of 75 grams of Dextrose (Glucose) powder in 300 ml of water on empty stomach in the morning and test the blood sugar after one hour. Show the result to your local doctor." -- T. Rama Prasad
DIABETES SCENARIO in 2024
Around November 14, 2024 ( WORLD DIABETES DAY ), media were flooded with information and advice on DIABETES. It helped some people to take preventive steps, and scared and stressed as well some people. Statistics showed that the diabetic population had grown globally four times in 30 years and that India got the dubious distinction of having the highest number of diabetics -- "The diabetes capital of the world". Though there may have been some flaws in arriving at the figures, the trend of rise of diabetes is evident. Of late, there has been a growing suspicion about the veracity of some of the rolled out statistics and the validity of conclusions of some research studies. Read my writing titled "MEDICAL LITERATURE" Go to https://drtramaprasad.blogspot.com/2017/03/medical-literature.htmlto know the unknown ! -- read it, it's only a click away. You may be surprised.
Based on scientific data, the government of India banned (suspended} the anti-diabetic drug 'Pioglitazone', and revoked the order within a month !!! Authentic studies concluded that a moderate consumption of alcohol in certain cardiac patients would be beneficial, and there are equally authentic studies which concluded that any quantity in any case is hazardous. If statistics and research data are to be believed,the following are the presently stated facts about DIABETES. Diabetes and obesity go hand in hand.
Obesity is a major public health problem worldwide which could not be brought down in spite of a tremendous build up of knowledge and its application. What's WRONG ? Can the new ANTI-DIABETIC drug TIRZEPATIDE set it RIGHT ? This injectable drug under the brand name MOUNJARO of Eli Lilly company costs around 1,000 US dollars per fill. It is expected to be available in the Indian market by 2025. The 'obesity drugs' market is expected to cross $100 billion in the next decade ! They would definitely reduce the weight in the pocket !!! In addition, TIRZEPATIDE is approved by the US FDA to treat OBSTRUCTIVE SLEEP APNEA (OSA) also.
(1) From around 200 million in 1990, the number of people with diabetes has quadrupled globally to over 800 million in 2022 while the global diabetes prevalence in adults rose from 7% to 14% between 1990 and 2022 (The Lancet, November 13, 2024). At 212 million, India has the highest number of people with diabetes as against China's prevalence of 148 million. India also topped the list of countries with 133 million people over the age of 30 years with untreated diabetes as against 78 million in China.
(2) Excessive eating (especially of unhealthy junk foods including processed, semi-processed and ultra-processed foods rich in sugars, fats, salts and calories) and decreased physical activity and the associated obesity are usually incriminated as the cause for the steep increase in diabetes. These factors are directly related to the increasing economic standards of the people. People are earning more, eating more fancy foods, consuming more food in hotels (of low quality), using more motorised vehicles, walking less, working less physically, spending more time with digital screens than outdoor games, and stressing themselves to achieve unrealistic material goals and living a bad lifestyle. They say : "What's life without eating and doing what we like ?." All these contribute to an increase in diabetes, obesity, hypertension, etc.
(3) People hate to be advised on DIETING & EXERCISE as it's hard to stick to good eating and working schedules. This is the main reason for the failure in diabetes management. And they don't like every illness they get to be linked to their diabetes just as any ill-defined health problem in aged persons is attributed to "age-related degeneration" !!!
(4) Diabetes or obesity is not just due to 'overeating' or 'under exercising'. We had seen people who eat tons of food and always glued to TV screens, and yet remain lean and lanky with normal blood sugar levels. Diabetes or obesity is related to complex ill-understood derangements in metabolism. Various predisposing factors for the causation of diabetes or obesity have come to the fore now --
(1) Excess fat deposition inside the abdomen, especially in the liver and pancreas. Fat metabolism seems to play as important a role as carbohydrate metabolism. Excess fat in liver leads to insulin resistance. A fat-loaded pancreas produces less insulin. Curiously, some babies born in India are found to be small in size though they have more fat than a normal proportion -- "Thin Fat Indian Child."
(2) Air pollution which acts as an endocrine disruptor, affects both the liver and the pancreas, and may produce diabetes. Air pollution provokes iinflammation that predisposes the body to cardio-metabolic diseases and visceral adiposity in the body. The ever-increasing air pollution may cause anything from cold to cancer.
(3) Genetic factors, which are not modifiable, may make one a diabetic. One very rare type of diabetes, called "Maturity Onset Diabetes of the Young (MODY) , is caused by a genetic mutation that affects insulin production and that is passed down through generations. Genetic testing reveals a mutation in HNFIA. Insulin therapy is not the answer to MODY. A C-peptide test may show adequate production of insulin, not consistent with Type 1 diabetes. MODY is not related to lifestyle.
(4) Epigenetic factors may impose the metabolic disorder.
(5) Deficiency of small adipocytes, especially in South Asians.
(6) Pregnant women's malnutrition, B12 deficiency and excess of folate in blood may trigger intrauterine programming of the foetus to develop diabetes in future -- diabetes non-genetically starting while still inside the womb !
(7) Gestational diabetes (diabetes starting during pregnancy) may persist later,.
(8) Childhood obesity or adulthood obesity may lead to diabetes and cardiovascular and renal diseases.
(9) Insufficient sleep may lead to hormonal imbalance and cause diabetes.
(10) And very importantly the neurohormonal influences of STRESS may promote diabetes. As though the stress of the modern life is insufficient, a new screening test is coming into vogue -- 1-h PG test (blood sugar one hour after a drink of 75 gm of glucose solution -- 75 gm of Dextrose monohydrate in 300 ml of water) to identify the risk of developing diabetes in future. Once this test tells that one may become a diabetic in the long future, the person may be stressed lifelong (akin to the Domicile's sword) even if she / he never becomes a diabetic !!! This stress itself may make one a diabetic or make one prone to a myriad of diseases. STRESS KILLS ! But the positive side is that one may take steps quite early and prevent becoming a diabetic. Read more about this test further below.
MANY TYPES of DIABETES
In addition to Type 1, Type 2, MODY (Maturity Onset Diabetes of the Young or HNIbeta mutations, a separate monogenic, autosomal dominant group of disorders) and LADA (mix of Type 1 and Type 2), we now have one more. "Type 5" diabetes is announced officially as a different entity at the International Federation Diabetes (IDF) at the World Congress of Diabetes 2025. People with Type 5 diabetes are typically underweight, have no family history of diabetes, have no antibodies related to Type 1 diabetes, not prone to ketoacidosis, and do not usually require insulin.
India is seeing a paradigm shift in diabetes understanding with the recognition of phenotypes such s Type 3 (connecting diabetes with Alzheimer's disease), Type (in lean, elderly folk), and Type 5 (owing to childhood malnutrition), all having atypical metabolic profiles.
REMEDY
Various advancements took place, including Stem Cell Therapy, in the management of diabetes. Notwithstanding, lifestyle changes will remain the cornerstone of managing diabetes. Going back to villages and living the good old lifestyle (eat well, work hard & sleep like a log) is an option which is not practicable !!!
BLUE CIRCLE is the 'Universal Symbol' for Diabetes
"Diabetes is a chronic disease that occurs either when the pancreas does not produce enough insulin or when the body cannot effectively use the insulin it produces. Insulin is a hormone that regulates blood glucose."
DIABETES and COVID-19
The impact of the COVID-19 pandemic on diabetes brought to the fore the research on this formidable duo. The evidence base is still a moving target even many years after the entry of the devastating virus. There is growing evidence that diabetics are at a higher risk of severe complications of COVID-19, and that the pandemic has substantially increased the diabetes burden on its own for unclear reasons (Rama Prasad. T., The Long COVID. The Antiseptic, 2022 October; Vol. 119; No. 10; P: 12-19;Indexed in IndMED –www.antiseptic.in ). Obesity may also be added to this duo -- the virus may be blamed directly or indirectly through the "lockdowns consequences."
It is well known that hyperglycaemia impairs defences and promotes infections. The interplay between diabetes and COVID-19 entails a complex pathophysiology which may lead to acute metabolic complications such as uncontrollable diabetic ketoacidosis and uncontrollable hyperglycaemia. To date, the mechanisms underlying the "conspiracy of this duo" are unclear. Nevertheless, it may be presumed that involvement of the Angiotensin Converting Enzyme 2 (ACE 2) receptors, a binding site for the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) is responsible. The ACE 2 is expressed in the key metabolic organ of diabetes, the pancreas -- especially the beta cells. This results in impairment in insulin secretion.
The virus may also precipitate Type 1 diabetes. In many of the cases of COVID-19, diabetic status got worsened, and in some cases diabetes had set in as a new problem. And, some patients on regular oral hypoglycaemic agents went out of control and had to be given insulin, without obvious history of contracting the virus. Were these cases infected with the virus and had the pancreas damaged, but didn't have any significant symptoms of Covid (many normal people are infected without the manifestation of any Covid symptoms) ? At present, there is no answer. To know more about this, look into my article : Rama Prasad. T., The Long COVID. The Antiseptic, 2022 October; Vol. 119; No. 10; P: 12-19;
The ominous and looming Corona and the trail of economic destruction it left in its wake has imposed a worldwide stress of humongous proportions. The resultant stress, anxiety, tension and depression is causing enormous morbidity and mortality across the world. Diabetes may be one of the diseases affected through neurohormonal influences of stress.
BAD LIFESTYLE
Owing to increasing bad lifestyle habits, diabetes has grown by leaps and bounds during the previous half-a-century. It remains to be seen as to how much more it would grow aided by SARS-CoV-2. Human physiology and pathology is a highly complex one, interlinked with all the systems in the body. Often, diabetics think that their problem is linked only to 'blood sugar'. In the same way, people diagnosed with many other diseases or disorders focus only on things related to those systems. Often, it's a combination of many abnormalities which may or may not show up as symptoms.
Anyway, some common things may be taken care of -- glycated haemoglobin (HbA1c) to be around 6.5 %; blood pressure around 130/80 mm/Hg; LDL cholesterol around 50 mg/dl; BMI around 25; Waist to Height Ratio (WHR) below 0.5 (waist circumference of less than half of the height).
Generally, a good lifestyle (healthy diet, adequate exercise ( and sleep, & low stress) ensures normalcy of these four parameters without medicines. These five things of 'good lifestyle' take care of not only diabetes but also of several other metabolic diseases. Of course, it's easier said than done in this 'MODERN WORLD' !!!
Diabetes mellitus, commonly known as diabetes, is a metabolic disease that causes high blood sugar. The hormone, insulin moves sugar from the blood into the body cells to be stored or used for energy. With diabetes, the body either doesn't make enough insulin or can't effectively use the insulin it does produce.
About 800 million people worldwide have diabetes, the majority living in low-and middle-income countries, and 1.6 million deaths are directly attributed to diabetes each year. Both the number of cases and the prevalence of diabetes have been steadily increasing over the past few decades.
OLD is GOLD !!!
Up to 1980s, we used to test blood sugar after giving a drink of glucose solution (Oral Glucose Tolerance Test or OGTT) to detect diabetes or predict the risk of developing diabetes. Later we have been using FPG, PPPG, HbA1c, MPG, etc. for that purpose, giving up the OGTT. Now, in 2024, the International Diabetes Federation (IDF) has recommended a simple 1-h PG test (blood sugar one hour after a drink of 75 gm of glucose solution -- 75 gm of Dextrose monohydrate in 300 ml of water) to roughly identify the diabetic status -- non-diabetic, Intermediate Hyperglycaemia (IH or Pre-diabetes or Impaired Glucose Tolerance - IGT) and Type 2 Diabetes (T2D) , setting aside HbA1c, FPG and PPPG of 2-hours. A level below 155 mg/dL is considered as normal, and a level above 209 as indicative of T2D. A level in between these two is IH or IGT or Pre-diabetes, indicating the possibility of becoming a diabetic in future. With the implementation of this recommendation, more "normal" people may come into the net of "diabetics", to the joy of some pharmaceutical and medical establishments !!! Some details of the recommendation are in the report below:
The 1-h PG test may be used to detect "future diabetics" with just one prick. The tests that are conventionally being used now for control of diabetes and detection of diabetes may continue to be employed.
The diagnostic spectrum has now extended from 'Visceral Fat' to 'Lipid Markers' to 'Gene Tests'.
'Fatty Liver Disease' often precedes diabetes and is now considered as a hepatic manifestation of 'Insulin Resistance'. Fatty Liver imaging, blood-based tests such as 'Validated Fibrosis' (to detect liver scarring) and 'Steatosis Scores (that quantify liver fat) can be imporrtant markers of diabetes risk. Body fat percentage, and visceral and ectopic fat measurement can provide a far better insight into metabolic risk than BMI figures. Triglyceride to HDL ratio, triglyceride-glucose index (TyG), and post-prandial lipid tests are also strong predictors of future diabetes and cardiovascular disease.
Retinal/iris AI scans, Body composition analysis, Homeostatic Model Assessment of Insulin Resistance (HOMA-IR), Triglyceride to HDL ratio (as a surrogate for insulin resistance and 'metabolic unhealthy obesity'), 1.5-Anhydroglucitol (1.5-AG) to detect PP spikes that HbA1c may miss, etc are some more tests that may detect diabetes early.
Continuous Glucose Monitoring (CGM) offers a powerful early tool, revealing post-meal excursions, glycemic variabilitty, and time-above-range long before conventional criteria are met with. While fasting insulin levels are a hallmark of Type 2 diabetes, offering insight into degree if insulin resistance, 'Hyperinsulinemic-Euglycemic Clamp Technique' remains the gold standard for assessing insulin sensitivity for the whole body. Althouugh glucose-based criteria are necessary for diagnosis, experts insist that in order to differentiate betweern types, clinicians must use context, history, phenotype, and autoantibodies or C-peptide tests, when needed.
BEWARE : A study (Lancet - Regional Health : Southeast Asia - 2026) showed that, in India's population, anaemia, haemoglobinopathies such as sickle cell disease and thalassemia, and glucose-6-phosphate dehydrogenase (G6PD) deficiency may distort annd affect glycated haemoglobin (HbA1c) values.
In those days, we used to monitor diabetics mostly by doing Benedict's Test (heating Benedict's reagent mixed with urine over an open flame). It's almost forgotten now.
With the country having the highest number of diabetic patients in the world, the disease is posing an enormous health problem to our country today. Often known as the diabetes capital of the world, India has been witnessing an alarming rise in incidence of diabetes (more than 200 million) according to data published in The Lancet of November 2024 / the International Journal of Diabetes in Developing Countries. According to a World Health Organization (WHO)'s fact sheet on diabetes, an estimated 3.4 million deaths are caused due to high blood sugar. And, diabetes is known to be associated with a number of disorders and diseases in the body.
REVERSAL of DIABETES
Sometimes, people are needlessly scared by showing statistics (true / false) or comforted by the very recent concept of 'REVERSAL' or 'REMISSION' of diabetes (this is now being debated).
Around 2023, the Internet is falloff promises to "reverse" diabetes, especially by using "Continuous Glucose Monitoring (CGM)" devices. These devices consist of a patch on the skin of arm which upon scanning shows instant level of blood glucose. It is without a needle prick and a glucometer. Otherwise it's the same mechanism used by the 'glucose strips'. As it is painless and very easy, it's more acceptable to the people to frequently monitor and adjust diet, exercise and medicines which may lead to better control. But, misleading ads and claims are made to reverse diabetes. One should be vary of the commercial gimmicks to sell CGMs and subscription plans for 'diabetes reversal'. Of course, in some milder forms of diabetes, there may be periods of "remission" (good control without medicines), not "reversal". This usually occurs following 'life-style' modification.
The latest & the futuristic
Emerging Role of AI in Diabetology
Diabetes accounts for an estimated 1.6 million deaths each year globally.
But there’s hope! Advances in diabetes management and healthcare have significantly improved mortality rates.
Artificial Intelligence (AI) is revolutionizing diabetes management through continuous glucose monitoring devices, offering real-time data to patients and healthcare providers, helping with immediate adjustments to insulin, and modifying dietary intake for better glycemic control. These proactive measures can improve diabetes management significantly.
To date, the advanced form of 'insulin injection' delivery is through an "open-loop" system made of electronics likened to 'artificial pancreas'.
Now, a "Smart Gel" is in the pipeline. This is a new user-friendly, electronics-free insulin delivery device that works like 'artificial pancreas' to distribute insulin in response to changing glucose concentrations. Researchers from the Tokyo Medical and Dental University have tested this design in mice. This "Smart Gel" uses a glucose-sensitive gel to deliver the appropriate amount of insulin through a catheter via a "closed-loop" approach. When the blood glucose levels are high, the gel becomes more permeable and releases more insulin, and when the glucose level is low, the gel develops a less permeable, skin-like layer to decrease insulin supply (Science Advances).
STEM CELL THERAPY
Chinese doctors claimed to have reversed Type1 diabetes in a 25-year-old woman in China with Stem Cell Therapy (2024). Long-term studies are going on and risks like immune rejection need to be understood. In the meantime, lifestyle changes will remain the cornerstone of managing diabetes.
We have developed a number of drugs and devices to control diabetes, but we couldn't find the exact cause which makes one a diabetic, except blaming the imperfect lifestyle or the genes. Perhaps, multiple factors are involved -- some known and some unknown ... even the toothpaste may be the one ! Researchers from the University of Texas found (2018) that crystalline particles of titanium dioxide were found in pancreas specimens from Type 2 diabetics. Titanium dioxide has become the commonly used white pigment in paints, food items, toothpaste, cosmetics, plastics and paper.
Are there any type 2 diabetes medicines that can help people lose weight and lower their blood sugar? Are there side effects?
There are two main groups of type 2 diabetes medicines that lower blood sugar and also may lead to weight loss. The first group is glucagon-like peptide 1 (GLP-1) agonists. The second is sodium glucose cotransporter 2 (SGLT-2) inhibitors.
GLP-1 agonists
GLP-1 agonists for type 2 diabetes are generally taken by a shot, also called an injection. Most are taken once a day or once a week. GLP-1 agonists include the following medicines.
Taken once a day by a shot:
Liraglutide (Victoza, Saxenda).
Lixisenatide (Adlyxin).
Taken twice a day by a shot:
Exenatide (Byetta).
Taken once a week by a shot:
Dulaglutide (Trulicity).
Exenatide extended release (Bydureon BCise).
Semaglutide (Ozempic).
Another form of semaglutide is available in a pill that's taken by mouth once a day. The brand name of that medicine is Rybelsus.
Tirzepatide (Mounjaro) is a similar kind of medicine called a dual-acting GLP-1/GIP agonist. It's also used to control blood sugar and can support weight loss. It is taken once a week by a shot.
All GLP-1 agonists can help with weight loss. But the amount of weight loss depends on the type of medicine and the dose. In general, studies have found that tirzepatide and semaglutide are the most effective for weight loss. Dulaglutide and liraglutide also have been found to be very effective. Other GLP-1 agonists appear to be somewhat less effective for weight loss. But people who take them still have better weight loss results than those who do not take the medicine.
GLP-1 agonists mimic the way a hormone called glucagon-like peptide 1 works in the body. When blood sugar starts to rise after a person eats, these medicines cause the body to make more insulin. The extra insulin helps lower blood sugar.
Lower blood sugar helps control type 2 diabetes. But it's not clear exactly how GLP-1 agonists lead to weight loss. They appear to curb hunger. They also slow the movement of food from the stomach into the small intestine. That means you may feel full faster and longer, so you eat less.
As with any medicine, there is a risk of side effects when taking a GLP-1 agonist. Some side effects can be serious. More common side effects often improve after taking the medicine for a while.
Common side effects include:
Nausea.
Vomiting.
Diarrhea.
Headache.
Low blood sugar is a more serious risk linked to GLP-1 agonists. The medical term for that condition is hypoglycemia. But the risk of low blood sugar typically only goes up when a person also is taking another medicine that's known to lower blood sugar. Examples include sulfonylureas and insulin.
GLP-1 agonists aren't recommended for people who:
Have had medullary thyroid cancer or who have a family history of the disease.
Have had multiple endocrine neoplasia or who have a family history of the disease.
Have had pancreatitis.
Are pregnant or are actively trying to get pregnant.
Are breastfeeding.
Certain GLP-1 agonists may not be appropriate for people who have a health condition that affects the intestines, such as gastroparesis, or for people who have some types of kidney disease.
Studies have linked GLP-1 agonists with certain thyroid tumors in rats. But until more long-term studies are done, the risk to humans isn't known.
SGLT-2 inhibitors
SGLT-2 inhibitors come in a pill that's taken once a day. They include the following medicines:
Canagliflozin (Invokana).
Dapagliflozin (Farxiga).
Empagliflozin (Jardiance).
Ertugliflozin (Steglatro).
Bexagliflozin (Brenzavvy).
These medicines work in the kidneys where they help take extra sugar out of the blood that then goes out of the body in urine. This lowers blood sugar. It also can help with weight loss. The weight loss benefits of SGLT-2 inhibitors typically are less than those of GLP-1 agonists.
Side effects of SGLT-2 inhibitors may include:
Genital yeast infections.
Urinary tract infections.
Lightheadedness.
Dizziness.
Nausea.
Kidney injury.
Weaker bones and a higher risk of broken bones.
A higher risk of diabetic ketoacidosis.
Rarely, SGLT-2 may be linked to a higher risk of infection in the feet and lower legs. If an infection is serious, it could lead to the need for amputation. People who have had wounds on their feet or other problems with their feet or lower legs should talk with their healthcare professionals about the possible risks before taking an SGLT-2.
SGLT-2 inhibitors aren't recommended for people who have had diabetic ketoacidosis. They also may not be a good choice for people with certain types of kidney disease.
Benefits beyond weight loss
Along with helping to control blood sugar and boosting weight loss, GLP-1 agonists and SGLT-2 inhibitors seem to have other health benefits.
Research has found that some of these medicines may lower the risk of certain serious health conditions, such as kidney disease, heart disease, heart failure and stroke. Many people who take these medicines also see their blood pressure improve. But it's not clear whether these benefits are from the medicine or a result of weight loss.
If you have type 2 diabetes and you want to find out if these medicines might be useful for you to lose weight, talk with your diabetes care team. They can help you decide what's best for your situation.
It was in 1967 .. half-a-century ago. I entered 'Perundurai Sanatorium' to join as a 'Medical Officer'. The first patient I saw was a case of 'Diabetic Foot' with 'Pulmonary Tuberculosis'. At that time, there were no 'Diabetologists' here around .. and there were not many diabetics .. we used to walk or cycle .. not much junk food .. a different lifestyle. During the 'Roman Empire' era, Galen, the Roman physician observed that he saw only two cases of diabetes in his entire career ! Lifestyle has changed a lot since then. This patient had to undergo amputation of the foot and also 'Thoracoplasty'. Patients were reluctant to have 'Insulin Injections', and doctors were also hesitant to prescribe the injections. Perhaps, 'modern therapy' could have saved his foot and the ribs. Even in those days, I used to 'scribble' something for publication. Hereunder are a few reprints of the published writings which are of 'archaic knowledge and of historical interest' at this point of time -- 2017 - 2024. They may hardly have any relevance to the present scenario. -- T. Rama Prasad
June 1980issue of the journal ANTISEPTIC. HIGHLY PURIFIED INSULINS -- an assessment. Author : Dr. T. Rama Prasad (more than 40 years ago when I used to type the articles on a manual typewriter and send them by 'Registered Post' ! )
Sept/Oct1981issue of the journal THE MEDICINE & SURGERY. DIABETES and TUBERCULOSIS.
Sept/Oct1981issue of the journal THE MEDICINE & SURGERY. DIABETES and TUBERCULOSIS.
January 14, 1983 issue of THE HINDU -- a comment on Prof. Ramdas's observation
NEW DRUGS in DIABETES in1998
FB id: T Rama PrasadReprinted from the FACEBOOK
DIABETES– new drugs… February 21, 2017
We just had a meeting of ‘Continuous Medical Education’ programme. I would not have posted this on FB as this is more of a pharmacological subject. But the home truths and the snide remarks about our drugs may be thought-provoking to the public and the doctor friends as well.
In my little talk at the meeting, I said something like the following:
“ … It is a refreshing experience to learn more about the age-old and important problem of ‘Diabetic Foot’. Thank you very much Dr. E. Thangavelu for enlightening us. This subject takes me down memory lane kindling nostalgic thoughts. It was half-a-century ago ( in 1967 -- most of you who are here now were yet to be born at that point of time ! ) when Ijoined as a Medical Officer at the ‘Perundurai Sanatorium’, and the first case I saw was a patient with ‘diabetic foot’ with gangrene and lung TB. There were no big corporate hospitals or diabetologists here around and there were not many alternative drugs to diabetes or TB. And today we are talking about ‘new’ anti-diabetic drugs while the incidence of diabetes and TB has been increasing enormously over the decades.
The world is currently having a great hope on the novel treatment of Type 2 diabetes by DPP-4 inhibitors. The status and the concern about the cardio-vascular safety of this new class of drugs is well-articulated by Dr. S.P. Hemanand. Thank you very much Dr. Hemanand for lucidly and comprehensively presenting the subject.
There are many DPP-4 inhibitors; some are in various stages of clinical development. The first approved DPP-4 was sitagliptin in 2006. Later, vildagliptin, saxagliptin, alogliptine, linagliptine, anagliptin and teneligliptin were introduced. Phase III studies are in progress with regard to more gliptins like denagliptin. The incretin agents (GLP-1 receptor agonists and the DPP-4 inhibitors) belong to a unique class of anti-diabetic agents.
There is a huge body of evidence of the goodness of DPP-4 inhibitors, beyond their hypoglycaemic effect. They have pleiotropic properties which improve b-cell function; reduce postprandial lipemia; lower blood pressure; improve myocardial contractility and endothelial function; and have potential neuroprotective, neurotrophic, and bone resorptive effects. These benefits of the incretins, if confirmed in long-term studies, have the potential to favourably influence the course of the disease process and its complications in patients with type 2 diabetes.
As the DPP-4 enzyme is involved not only in the regulation of glucose but also several substrates like BNP, brain natriuretic peptide; SDF-1, type 1 stromal derived factor; NPY, neuropeptide; PYY, peptide YY, DPP 4 inhibitors may have cardio-protective benefits and immune-modulating actions. Thus, they favourably modify myocardial contractility, blood pressure, cardiac output, etc. ALL THIS IS MUSIC TO THE MANUFACTURERS.
Now, let us turn to the flip side of the issue. These new drugs are ‘validated regarding surrogate outcomes’ but not about ‘real-world outcomes’. Sometimes, adverse evidence comes a bit late, often due to vested interests. Often, the “pro-industry ‘paid’ cacophony” overshadows reports of adverse reactions. Some drugs once considered to be ‘most effective and least toxic’ are now banned. Evidence is now growing to list some statins as dangerous drugs. We don’t know about the durability or long-term safety of the DPP 4 inhibitors. The jury is still out on DPP-4 inhibitors. Let us wait and see. AND, THIS IS A BITTER PILL TO THE BIG BUSINESS BARONS.
All said and done, the world is running on money, including research. The big business barons go to any extent, laughing all the way to the bank. These days, scientific evidence may be genuine or fabricated, what with all the talk about “paid research.” The evidence is too much to ignore. This reminds me of a scientific flip-flop in India. The diabetic drug, pioglitazone was ‘banned’ in India in 2013. And the government made a ‘U-turn’ and the ‘ban’ was revoked within weeks. Can any one of you tell me why such a laughable lapse occurred ? It was alleged that a DPP-4 inhibitor drug was behind the ban of pioglitazone ! There were allegations in the media and medical circles that the reason behind the ‘ban’ was based on adverse reports (bladder cancer) on pioglitazone from a diabetes research institution in India which received funds from a medical company whose new diabetes drug sitagliptin stands to gain if pioglitazone was banned. Do you think that there are genuine and scientific reasons behind the decisions ? You bet not. Lies, damned lies and drugs !
I wrote about many of such murky deals in my article titled “MODERN MEDICINE – how good is it in India ?” You may get that article by writing to me over my E-mail. It was published in the ‘Co-Chamber Journal (The Indian Chamber of Commerce and Industry)’. … ”
“Unless the thief decides to transform himself, it is never possible to eradicate stealing.”(“thirudanai parthu thirunthavital thirutai olika mudiyathu.”)
-- Pattukottai Kalyanasundaram
Dr. T. Rama Prasad, drtramaprasad@gmail.com, 'PAY WHAT YOU CAN’ Clinic, Perundurai, Erode Dt., TN, India., Former Medical Superintendent (Special), RTS & IRT Perundurai Medical College and Research Centre.
Reprinted from the FACEBOOK
DIABETIC FOOTJuly 9, 2017
I have just returned from a Symposium on the above subject. Many people pay 'low' attention to their feet, perhaps, as they are 'low down' ! Diabetics should pay adequate attention to their feet (more than the face which is 'high up'). Otherwise, even a minor injury may make the feet end in complications. Foot has a low status in human minds. We profusely apologise when accidentally our foot just touches any part of anybody, even their foot .. but not when our hand touches.What a partiality !Foot does more strenuous work than the hand .. hence, we have “Diabetic Foot” (disease), but not “Diabetic Hand” !But, paradoxically, we touch the feet of somebody to express our reverence and respect, and to seek blessings ! A conundrum !Anyway, please respect the foot. You may read about 'new' drugs in diabetes on my blog - Dr. T. Rama Prasad's Scribblings--https://drtramaprasad.blogspot.com. – under the title ‘DIABETES’.
I had asked one of the speakers, in a lighter vein, as to whether diabetic foot problems are more in the right foot or the left. He couldn't cite any data. Traditionally, we are advised to put the right foot first, while entering a house or going up the steps. I was wondering whether the practice of always 'starting off on the right foot' makes the right foot more vulnerable to injuries andinfection !
Feet have long been the subject of superstition. A mole on the sole of the left foot is said to be inauspicious. When the right foot itches, a happy travel is predicted. The right foot is associated with a positive vibe.
The tennis star, Rafael Nadal was always found to put his right foot first while leaving or entering a tennis court without touching the lines. See the video -- file:///Users/ramaprasadtata/Pictures/Tennis.html.
Dr. T. Rama Prasad,Perundurai.
SUGAR STRENGHTHENS ROADS !!!
So, diabetics must be stronger !!!
At an international conference in Malaysia on "Road engineering in Asia and Australia", in 1973, presentation of a scientific study showed that addition of SUGAR to cement increased the strength and durability of roads. That was 'fifty years ago''. Now, it seems that science, sometimes, is to be taken with a pinch of salt to savour its sweetness !!! Science or nonsense !
COMMENTS Raghu Rangaswamy Hi Dr. I do accept your comments. It’s sad to say many drugs which are banned abroad citing various proven evidences are still marketed in India, which clearly indicates money can do anything in this country. I have no idea who will tie the bell to these mafias. I appreciate the recent Govt's action on bringing down the cardiac stent prices by 80% lower, the same thing should be brought on medicines too. Being in medical research I would say every medicine you take is a chemical and it’s not going to give you miracle. They bind to certain receptors which are responsible for a disease, but one can't assure the same chemical will not bind to other receptors and block the natural body function. The reason is body produces few chemicals which interacts with many receptors. For example ATP binds to nearly 300+ kinases which are involved in different body functions, when you design a kinase inhibitor even though your molecule binds to your desired kinase but it will also bind to other kinases because of the protein structural similarity. The best way one should do is to have control on the food, to change life style and to prefernatural remedies. Being in modern medicine profession, I will still give my vote to ayurveda and naturopathy. I still vouch that our ancestors were more knowledgeable than today’s technologically advanced scientists. I wonder how they identified certain herbs and plants for diseases.
Sivaraman Subramanian What a wonderful article sir ! ...Great depth of knowledge, in-depth understanding of the real situation...Great eye-opener sir.. Thanks Sir.
Solaiappathevar Narayanan Thank you Dr. T. Rama Prasad garu for your thought- provoking article. Now, can we hope to get the desired results through stem cell therapy enhancing Beta cells of Islets of Langerhans which produce chiefly insulin. This can help overcome insulin resistance. Our native herbal medicines should be encouraged on scientific lines.
Muthu Raja sir,i still remember the visual aid and detailing talk about tolbutamide in the year 1978.the drug metformin which is widley in use today launched after long delay in 1974.sir,you are the only doctor who has the guts to write about the real reason behind the ban of pioglitazone. All the formulations are sold with doctors prescription.Pattukottaiyar rightly said thirudanai parthu thirunthavital thirutai olika mudiyathu..
Sridhar Vatyamkumaraswami Having been in pharma marketing for about 30 years,I concur with you.Today's medico marketing is one sided.They have been bothered about converting or convincing some opinion builders,a small section of Doctors whose prescriptions are followed.
Inhibition of dipeptidyl peptidase 4 (DPP-4) is a novel treatment for type-2 diabetes. DPP-4 inhibition prevents the inactivation of glucagon-like peptide 1 (GLP-1), which increases levels of active GLP-1. This increases insulin secretion and reduces glucagon secretion, thereby lowering glucose levels. Several DPP-4 inhibitors are in clinical development. Most experience so far has been with sitagliptin (Merck; approved by the FDA) and vildagliptin (Novartis; filed). These are orally active compounds with a long duration, allowing once-daily administration. Both sitagliptin and vildagliptin improve metabolic control in type-2 diabetes, both in monotherapy and in combination with metformin and thiazolidinediones. A reduction in HbA(1c) of approximately 1% is seen in studies of DPP-4 inhibition of up to 52 weeks' duration. DPP-4 inhibition is safe and well tolerated, the risk of hypoglycaemia is minimal, and DPP-4 inhibition is body-weight neutral. DPP-4 inhibition is suggested to be a first-line treatment of type-2 diabetes, particularly in its early stages in combination with metformin. However, the durability and long-term safety of DPP-4 inhibition remain to be established.
Acts when sugar increases after a meal, increases insulin levels (help lower blood sugar) and decreases glucagon (a hormone that raises blood sugar) Linagliptin (Trajenta™), Saxagliptin (Onglyza®), Sitagliptin (Januvia®) Combination agents: Linagliptin/metformin (Jentadueto®), Saxagliptin/metformin (Komboglyze™), Sitagliptin/metformin (Janumet®)In the future further gliptins (alogliptin, linagliptin, denagliptin) may be marketed, with which Phase III studies are in progress or the results have already been published. . At present, there seems to be little to distinguish between the different inhibitors in terms of their efficacy as antidiabetic agents and their safety. Long-term accumulated clinical experience will reveal whether compoundrelated characteristics lead to any clinically relevant differences.
P 1 analogues; incretins I. INTRODUCTION DPP 4 (dipeptidyl peptidase-4) inhibitors are the recently developed and approved chemical for the treatment of the diabetes mellitus. They act mainly on pancreas via inhibition of degradation of the incretin hormones such as type 1 glucagon like peptide (GLP-1), and GIP. The Incretin hormones are release from the intestine in response to oral glucose ingestion and stimulate insulin release from β-cells of pancreas (so called incretin effect), and also suppress glucagon release from α-cells of pancreas. DPP-4 inhibitors are approved for the treatment in Type 2 diabetes either as monotherapy or as add-on therapy with other oral hypoglycemic agents like metformin. There are numerous DPP4 inhibitors; some are in various stages of clinical development. The first approved DPP4 was sitagliptin in 2006. Then vildagliptin, saxagliptin, alogliptine, linagliptine, anagliptin and teneligliptin were introduced.
es like Parkinson’s disease and alzeimer disease. IX. CONCLUSION The incretin agents (GLP-1 receptor agonists and the DPP-4 inhibitors) belong to a unique class of antidiabetic agents. These agents have pleiotropic effects that extend beyond their known ability to lower glucose. These include effects to improve b-cell function and mediation of trophic effects on the b-cell (in animal and in vitro models); effects to reduce postprandial lipemia; effects to lower blood pressure; effects to improve myocardial contractility and endothelial function; and potential neuroprotective, neurotrophic, and bone resorptive effects (seen only in animal models). These beneficial effects of the incretins (if confirmed in longterm studies) have the potential to favorably influence the course of the disease process and its complications in patients with type 2 diabetes.
DPP 4 (dipeptidyl peptidase-4) inhibitors: beyond glycemic control 83 III. CARDIOVASCULAR PROTECTION Effect on Myocardial function Heart failure, myocardial infarction, cardiac hypertrophy and coronary artery disease is often associated with diabetes and metabolic syndrome. As the DPP-4 enzyme is involved not only in the regulation of glucose but also several substrates (like BNP,brain natriuretic peptide; SDF-1, type 1 stromal derived factor; NPY, neuropeptide; PYY, peptide YY) known to have cardiovascular, renal and immune-modulating actions. Thus long-term DPP-4 inhibition may have clinical benefits and/or consequences including cardioprotective actions. Effects on contractility, blood pressure, cardiac output and cardioprotection appear to be independent of diabetes [12-19] . A few studies have been published on cardioprotective effect of GLP-1 analogues and DPP 4 inhibitors. In studies done on mice genetically lacking the DPP-4 receptors that were treated with sitagliptin, the investigators induced acute myocardial infarction by left anterior descending coronary artery ligation (20). In these mice, an upregulation of cardio-protective genes and their protein products was shown. In another study in mice, it was shown that treatment with sitagliptin can reduce the infarct area and the protective effect of sitagliptin was protein kinase A dependent (21) . In diabetic patients who suffer from ischemic heart disease, it was demonstrated that treatment with sitagliptin improved their heart function and coronary artery perfusion, as observed in echodebutamin tests (22) . IV. EFFECT ON BLOOD PRESSURE The effect of DPP 4 inhibitors on blood pressure is contradictory. In diabetic rats, sitagliptin was associated with a significant normalization of blood pressure in diabetic rats with elevated blood pressure (versus non-diabetic rats)(23) , whereas vildagliptin showed no influence on blood pressure in hypertensive fatty rats (24). Recently, a study by Marney et al.(25), in metabolic syndrome patients, showed that during placebo and low-dose ACE inhibition (5 mg enalapril), sitagliptin lowered blood pressure. However, this trend was reversed during higher-dose acute ACE inhibition (10 mg enalapril). They hypothesized that the combination of sitagliptin and high-dose ACE inhibition causes activation of the sympathetic tone, hence attenuating blood pressure reduction. Marney et al. suggested that high levels of substance P, because of the double blockade of ACE and DPP-4, caused the activation of the sympathetic system. V. ENDOTHELIAL FUNCTION Endothelia dysfunction is an independent predictor for cardiovascular events in patients with type 2 diabetes. In some studies it was found that GLP-1 has some vasodilatory action and Sitagliptin significantly improved endothelial function and inflammatory state in patients with coronary artery disease and uncontrolled diabetes mellitus. VI. LIPID METABOLISM DPP 4 inhibitors found to decrease the postprandial surge in lipid levels. Matikainen et al.(26) in his study found that treatment with vildagliptin for 4 weeks improves postprandial plasma triglyceride and apolipoprotein B-48–containing triglyceride-rich lipoprotein particle metabolism after a fat-rich meal in drugnaive patients with type 2diabetes. Hsieh et al. (27) also suggested that DPP 4 inhibitors augment the level of GLP-1receptors thus reduce secretion of tryglycerol, cholesterol, and apolipoprotein B-40 from intestine. Antiatherosclerotic effect has been found in some model by reducing media-intima ratio in carotid artery of rat in dose dependent manner.
ulature. 3.4 Cardiovascular effects Although it summarized the results of studies with non-cardiovascular endpoints, a metaanalysis investigating the safety of sitagliptin (100mg/day) showed no substantial differences as compared to the control group in relation to coronary artery disease (0.2 vs. 0.4 event per 100 patient-years), myocardial ischemia (0.0 vs. 0.2 event per 100 patient-years) and acute myocardial infarction (0.1 vs. 0.2 event per 100 patient-years) respectively (Williams-Herman, Engel et al. 2010). A post hoc metaanalysis of saxagliptin’s effect on major cardiovascular events (CV death, non-fatal MI, non-fatal stroke) showed no increase of CV risk in the treated patients (Wolf, Friedrich et al. 2009). Recently, a large outcome trial with sitagliptin (A randomized placebo controlled clinical Trial to Evaluate Cardiovascular Outcomes after treatment with Sitagliptin in patients with type 2 diabetes mellitus and inadequate glycaemic control on mono or dual combination oral antihyperglycaemic therapy, TECOS) and with saxagliptin (Saxagliptin Assessment of Vascular Outcomes Recorded in patients with diabetes mellitus, SAVOR-TIMI 53) has been started. GLP-1 receptors can be found in cardiac muscle cells and vascular endothelial cells as well (Nauck and Smith 2009; Nikolaidis, Mankad et al. 2004). The beneficial effect of GLP-1 has been demonstrated also in coronary ischemia and left ventricular failure both in animal experiments and in human studies (Nikolaidis, Mankad et al. 2004; Bose, Mocanu et al. 2005; Nikolaidis, Elahi et al. 2004). In rats, myocardial necrosis developed in a smaller area when they received GLP-1 infusion (Bose, Mocanu et al. 2005). Following intravenous infusion of GLP-1, less wall motion disorder and better left ventricular function developed in patients with and without type 2 diabetes who had undergone angioplasty after acute myocardial infarction (Nikolaidis, Mankad et al. 2004). Based on these, a beneficial effect of DPP-4 inhibitors on cardiovascular disease may be presumed, however further long-term clinical studies with a high number of patients are required for an exact elucidation. www.intechopen.com
In addition to severe joint pain, other possible side effects of DPP-4 inhibitors include inflammation of the pancreas, low blood sugar when this class of medicines is combined with other prescription medicines used to treat diabetes, and allergic reactions. =====================================================================
The following is a list of some of my 'scribblings', including a few from the 28 articles on COVID published in a monthly medical journal in 30 months (a world record). To open them, click on any of the titles. -- T. Rama Prasad
These are only scribbles for the general audience to pass some time, not for experts. The expressions may be biased and the narration may be a crashing bore on negative aspects. Taste a bit of the bitterness before leaving. -- T. Rama Prasad
During my childhood, one of my schoolmates had huge nails. Her name was Gowri. We nicknamed her as ‘Goru’ (‘goru’ in Telugu means nail of a finger or toe ). They used to say that her huge nails caused a problem in her heart. It might be a case of ‘Digital Clubbing’ (abnormal nails present in some ‘Congenital Heart Diseases’). After one summer vacation, ‘Goru’ didn’t come back to the school. It was learnt that she died due to the nail / heart problem, and that treatment could not be availed as they didn’t have money to pay for it.
Perhaps, this incident prompted me to look at everyone’s nails from that time which might have led me to report the first casefrom India of ‘Yellow Nail Syndrome (YNS)’ from India in 1980 (published in an American journal, CHEST) and the first case in the world of ‘Yellow nails & Covid’ in 2023, published in an Indian journal, THE ANTISEPTIC - https://drtramaprasad.blogspot.com/2017/04/yellow-nail syndrome_28.html
And perhaps, the preventable death of ‘Goru’ due to the inability to pay for the treatment motivated me to start my ‘PAY WHAT YOU CAN’ Clinic (PWYCC) half-a-century ago where patients may pay whatever they can. No fixed fee ( http://drtramaprasad.blogspot.com/2017/06/pay-what-you-can-clinic.html ). The credit for these case reports on YNS and the starting of my PWYCC should go to ‘Goru’. Thanks to “Goru”.
( Translated by Prof. B.M. Hegde as: “Rejoice in giving.”)
True to this quote, I have been rejoicing at what little I could give. Defying stereotypes, this clinic has been in existence for a very long time, sans glitz, blitz, ads, microphones, speeches and noise. As a matter of my policy, publicity is shunned. The reason is simple. Good work needs no noise and nonsense. My ‘SCRIBBLINGS’ on related topics may be accessed at:http://drtramaprasad.blogspot.com
My consultation fee is not decided by me. It is the patient’s pleasure. The patient may pay (donate) whatever he can and what he wishes. If one is short of money, he or she need not pay anything. The money may just be put into the ‘hundi’ box kept outside the consultation room. And the money thus received is used for charity to help the needy, the poor and the less fortunate.If interested to know more about this facility, go to:http://drtramaprasad.blogspot.com/2017/06/pay-what-you-can-clinic.html. And, if you wish, you may also 'contribute what you can' through bank (Dr. RAMA PRASAD T, A/C No. 451075868, INDIAN BANK, IFS CODE IDIB000P155, PERUNDURAI, Erode District, Tamil Nadu - 638052 ).
"We need not run after money. If we are meritorious and compassionate, money would run after us, and it eludes us if we run after it.” -- T. Rama Prasad
“Richness is not having lots of money. It is the feeling that one has enough of it. Contentment sans comparison is what makes one really rich.” -- T. Rama Prasad.
As soon as we obtained on your web site despite the fact that obtaining thing to consider essentially fairly little bit submits. Enjoyable technique for forthcoming, I'm book-marking simultaneously obtain types finish increases up-wards. click here
Roche’s Chemist understands that most of you are completely dependent on your blood glucose meter as it helps you to conduct blood glucose test for diabetes from the comfort of your home. We feel privileged to serve you with the best quality of diabetes test kit and lancets online.
Great, there's so much information to know even I didn't even know few things that I found here. This website PCD Pharma also provides so much knowledge about PCD Pharma.
Dear Sir , Your article on Diabetes and Corona in a person very interesting , amazing and persistently writing to the society and medical professionals and thought provoking. So that each and every patient along with history of Diabetes we also ask Corona vaccination done and how many injections given and affected by corona viral infection before or after vaccination .
Nice blog! Thanks for sharing this blog. PlatinumRx provides access to the best diabetes medicines in India, trusted by healthcare professionals for their efficacy and safety. Visit us today!
Tastiq DM is a sugar-free cough syrup specially formulated for diabetic individuals. It helps relieve cough without affecting blood sugar levels, making it a safe and effective choice for managing cold symptoms in diabetes.
Great post! The growing interest in Mounjaro for weight loss really highlights how far we've come in supporting people on their health journeys. It's encouraging to see real results backed by science, and it’s exciting that more individuals have access to effective treatments like this
Insightful blog! Obesity and diabetes are deeply connected, and regular tests like HbA1c , fasting blood sugar, and lipid profile are crucial for early detection and management.
Awesome post! With the growing demand for effective weight loss solutions, it's great to see how accessible options likeMounjaro online have become. The convenience of getting expert guidance and treatment from home is a game-changer for so many people.
I’ve been living with Parkinson’s disease for some time, and nothing I tried seemed to make a lasting difference—until I began the herbal treatment from NaturePath Herbal Clinic. I was skeptical at first, but after about four months, I started to notice real improvements. My tremors became less frequent, my stiffness reduced, and my balance and coordination gradually began to improve. For the first time in years, I feel more in control of my body and daily life. I can move more freely, sleep better, and even enjoy simple activities again without constant discomfort. The changes have been truly uplifting—both physically and emotionally. If you're exploring natural options for managing Parkinson’s, I genuinely recommend giving this a try. It’s been a life-changing experience for me. Learn more at: www.naturepathherbalclinic.com
I want to use this opportunity to testify of the marvelous work of Dr. Isaac and how he has helped me in curing my sickness and bringing happiness into my life. I can really vouch for Dr. Isaac in herbal treatment. I was suffering from diabetes, Cervical Cancer and infected with HPV and Herpes. I used to have incessant bleeding and there was nothing I could do until a childhood friend introduced me to Dr. Isaac Remedies. I spoke with him and ordered his recommended medication which was delivered to me through DHL. Immediately I began using the herbal medicine, within 2 weeks I couldn't feel any pain. It took me 6 weeks to finish the medicine and afterwards I was completely cured. I highly recommend that you contact him to help you at his email drisaacherbscure2@gmail.com OR What'sApp/Call him at +234 8075449538. Thank you so much sir for what you did for me you are the best of all. TEXT OR WhatsApp: +234 80 7544 9538.
Nice Article! I’ve read that injectable NAD for sale helps with cell repair and recovery. When looking for NAD injections for sale, always verify the provider’s certifications.
I had visited your website. You did a great job of creating this. It looks beautiful and full of creativity. I appreciate your efforts on this website.
I found this blog incredibly helpful and easy to understand, especially the way complex points were explained so clearly. It provided practical insights that readers can actually apply in real life. The structure and flow of the content made it engaging from start to finish. Really loved the insights shared in this blog—very informative and well-written. Keep up the great work! If anyone’s looking for topics related this blogDiabetes Mellitus Treatment in Ghatkopar
This was a very informative post and I liked how you explained the connection between obesity, lifestyle, and diabetes in simple words. It reminds us that small daily habits can have a big impact on our health. Following a proper diabetes remission diet along with regular activity may help people make better choices. Thank you for sharing such valuable awareness.
Dr. Prasad’s insights on "Diabesity" highlight how complex metabolic management has become with these new medications. It's crucial for patients to find a specialized endocrinologist queens blvd to safely navigate these chronic conditions and lifestyle changes effectively.




















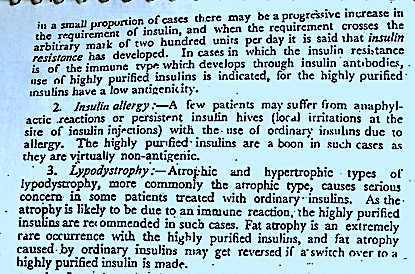













 I had asked one of the speakers, in a lighter vein, as to whether diabetic foot problems are more in the right foot or the left. He couldn't cite any data. Traditionally, we are advised to put the right foot first, while entering a house or going up the steps. I was wondering whether the practice of always 'starting off on the right foot' makes the right foot more vulnerable to injuries and infection !
I had asked one of the speakers, in a lighter vein, as to whether diabetic foot problems are more in the right foot or the left. He couldn't cite any data. Traditionally, we are advised to put the right foot first, while entering a house or going up the steps. I was wondering whether the practice of always 'starting off on the right foot' makes the right foot more vulnerable to injuries and infection ! 






As soon as we obtained on your web site despite the fact that obtaining thing to consider essentially fairly little bit submits. Enjoyable technique for forthcoming, I'm book-marking simultaneously obtain types finish increases up-wards. click here
ReplyDeleteRoche’s Chemist understands that most of you are completely dependent on your blood glucose meter as it helps you to conduct blood glucose test for diabetes from the comfort of your home. We feel privileged to serve you with the best quality of diabetes test kit and lancets online.
ReplyDeleteGreat, there's so much information to know even I didn't even know few things that I found here. This website PCD Pharma also provides so much knowledge about PCD Pharma.
ReplyDeleteDear Sir ,
ReplyDeleteYour article on Diabetes and Corona in a person very interesting , amazing and persistently writing to the society and medical professionals and thought provoking.
So that each and every patient along with history of Diabetes we also ask Corona vaccination done and how many injections given and affected by corona viral infection before or after vaccination .
Nice blog! Thanks for sharing this blog. PlatinumRx provides access to the best diabetes medicines in India, trusted by healthcare professionals for their efficacy and safety. Visit us today!
ReplyDeleteNice Post!!
ReplyDeletePlease Look Here At Pediatric Pre Diabetes Program
Tastiq DM is a sugar-free cough syrup specially formulated for diabetic individuals. It helps relieve cough without affecting blood sugar levels, making it a safe and effective choice for managing cold symptoms in diabetes.
ReplyDeleteGreat post! The growing interest in Mounjaro for weight loss really highlights how far we've come in supporting people on their health journeys. It's encouraging to see real results backed by science, and it’s exciting that more individuals have access to effective treatments like this
ReplyDeleteInsightful blog! Obesity and diabetes are deeply connected, and regular tests like HbA1c , fasting blood sugar, and lipid profile are crucial for early detection and management.
ReplyDeleteAwesome post! With the growing demand for effective weight loss solutions, it's great to see how accessible options likeMounjaro online have become. The convenience of getting expert guidance and treatment from home is a game-changer for so many people.
ReplyDelete
ReplyDeleteI’ve been living with Parkinson’s disease for some time, and nothing I tried seemed to make a lasting difference—until I began the herbal treatment from NaturePath Herbal Clinic. I was skeptical at first, but after about four months, I started to notice real improvements. My tremors became less frequent, my stiffness reduced, and my balance and coordination gradually began to improve.
For the first time in years, I feel more in control of my body and daily life. I can move more freely, sleep better, and even enjoy simple activities again without constant discomfort. The changes have been truly uplifting—both physically and emotionally.
If you're exploring natural options for managing Parkinson’s, I genuinely recommend giving this a try. It’s been a life-changing experience for me.
Learn more at: www.naturepathherbalclinic.com
I want to use this opportunity to testify of the marvelous work of Dr. Isaac and how he has helped me in curing my sickness and bringing happiness into my life. I can really vouch for Dr. Isaac in herbal treatment. I was suffering from diabetes, Cervical Cancer and infected with HPV and Herpes. I used to have incessant bleeding and there was nothing I could do until a childhood friend introduced me to Dr. Isaac Remedies. I spoke with him and ordered his recommended medication which was delivered to me through DHL. Immediately I began using the herbal medicine, within 2 weeks I couldn't feel any pain. It took me 6 weeks to finish the medicine and afterwards I was completely cured. I highly recommend that you contact him to help you at his email drisaacherbscure2@gmail.com OR What'sApp/Call him at +234 8075449538. Thank you so much sir for what you did for me you are the best of all. TEXT OR WhatsApp: +234 80 7544 9538.
ReplyDeleteNice Article! I’ve read that injectable NAD for sale helps with cell repair and recovery. When looking for NAD injections for sale, always verify the provider’s certifications.
ReplyDeleteI had visited your website. You did a great job of creating this. It looks beautiful and full of creativity. I appreciate your efforts on this website.
ReplyDeleteNatural Agave Sugar Substitute
I found this blog incredibly helpful and easy to understand, especially the way complex points were explained so clearly. It provided practical insights that readers can actually apply in real life. The structure and flow of the content made it engaging from start to finish. Really loved the insights shared in this blog—very informative and well-written. Keep up the great work! If anyone’s looking for topics related this blogDiabetes Mellitus Treatment in Ghatkopar
ReplyDeleteThis was a very informative post and I liked how you explained the connection between obesity, lifestyle, and diabetes in simple words. It reminds us that small daily habits can have a big impact on our health. Following a proper diabetes remission diet along with regular activity may help people make better choices. Thank you for sharing such valuable awareness.
ReplyDeleteDr. Prasad’s insights on "Diabesity" highlight how complex metabolic management has become with these new medications. It's crucial for patients to find a specialized endocrinologist queens blvd to safely navigate these chronic conditions and lifestyle changes effectively.
ReplyDelete