
INDIAN IMMUNITY, BCG VACCINATION and COVID
About the author :
Dr. T. Rama Prasad is the WORLD RECORD holder of authoring 28 articles related to COVID-19 in 30 months, published in a medical journal (The Antiseptic – www.theantiseptic.in -- Indexed in IndMED), and reporting in the same journal the WORLD’s FIRST CASE of ‘Yellow Nail Syndrome’ associated with COVID-19, PT & DM (https://drtramaprasad.blogspot.com/2017/04/yellow-nail syndrome_28.html ). He wrote his first article in the premier journal, The Antiseptic, four decades ago. Many of his articles written over half-a-century may be accessed at https://drtramaprasad.blogspot.com/2017/04/dr-t-rama-prasad.html & https://drtramaprasad.blogspot.com/2017/04/my-in-newspapers_28.html & https://drtramaprasad.blogspot.com .
He is the former MEDICAL SUPERINTENDENT (Special) of R.T. Sanatorium & Perundurai Medical College and Research Centre. Presently, he is the Senior Consultant in TB & Lung Diseases, and the Director at ‘PAY WHAT YOU CAN’ Clinic, Perundurai, He is the recipient of the “Lifetime Achievement Award” of the ‘Coimbatore Respiratory Society’, and the honorific title “Perundurai Rathinam” from the body of ‘Perundurai Public’.



April 2026: Don't get scared by knowing that a new COVID-19 variant, nicknamed as 'CICADA', is spreading fast in the US and parts of Europe over the past one month (March 2026), primarily affecting children. So far it has not seriously impacted health. We, INDIANS, need not be afraid of this new variant as we are lucky in having "INDIAN IMMUNITY." The COVID-19 virus is continually making changes to its genetic structure, so that it can escape being detected by existing human immune responses that were based on earlier versions of the virus. The earlier versions of the virus might have lived in a person of reduced immunity for a long time, gradually accumulating one mutation at a time.

April 1
You are an Indian and you had BCG vaccination. And you had grown up amidst filth and germs. So, you may be immune to COVID-19.
No, it's not an APRIL FOOL'S DAY joke (today is April 1). COVID-19 has spread to most countries across the globe. Puzzlingly, the impact of the disease is different in different countries. Why ? We don't exactly know. Cultural norms, food habits, climate, affluence, empowerment, infrastructure, mitigation efforts, etcetera are cited as possible reasons for the differences. Two more factors may be added to the strength of very recent studies. 1. Indian immunity. 2. BCG vaccination.
One glaring example is this. Compare India and the US. India is very weak in healthcare compared to the US. India's population is enormous at 140 crores while the US population is just 30 crores. Americans could get vaccinated quite early and that too by the world's best-rated vaccine, mRNA. Notwithstanding the aforementioned factors, only 5 lakhs of people died due to COVID in India whereas 12 lakhs of deaths occurred due to COVID in the US. And, India's 'COVID Death Rate' per million of population is quite low, less than half of the average of the countries where BCG had not been given as a routine. Why did this unexpected phenomenon occur ? What protected the Indian population ??? That the statistics are flawed and don't reflect the ground realities, and that the registration of deaths in the US has been perfect (leading to the dubious distinction of the US in scoring a high rate of deaths !) is a moot point. Moreover, definition of "COVID DEATH" is not uniform in all the countries. Even if all these are factored in, the low level of impact on Indians is glaring. For a deeper understanding of the 'COVID deaths' and the controversies about the recording of the deaths, go to my article titled "COVID DEATHS" -- The Antiseptic, Vol 119, No 7, July 2022, www.antiseptic.in ; Indexed in IndMED.
1. INDIAN IMMUNITY and WESTERN VULNERABILITY
Our environment is full of filth, bacteria and viruses. So, we had a lot of subclinical (not very symptomatic and not compelling to see a doctor) infections which generated immunity (resistance) -- like racial or herd immunity, over a period of decades and centuries. Lower resistance in western societies may curiously be due to over sanitisation (too much of cleanliness and hygiene). If a little is good, a lot need not necessarily be better. This concept may be strange and unacceptable, but this view may be vindicated by 'post-corona' epidemiological studies. The Indian food habits and the Indian lifestyle might also have played a part.
Curiously, the Supreme Court, on Dec 18, 2025, found no sense in a plea to further purify packaged drinking water to meet with Western standards, saying that many in India struggle to get ordinary drinking water and that people in rural areras had been drinking ordinary groundwater for ages, and nothing happened to them, and that the court could not lose sight of broader realities faced by the people. The court dismissed the case as that of a 'Luxury Litigation'. This could be an example of INDIAN IMMUNITY.


We all have thousands of microbes in our bodies which may not produce disease because of our immunity. And, in course of time, we may naturally gain immunity, called ‘herd immunity’, to this coronavirus also, through subclinical infections. When around 65% of the population has antibodies, presumably due to infection (asymptomatic or symptomatic), it may be assumed that the population has gained herd immunity. As on August 20, 2020, we have the jaw-dropping sero-survey results -- 57% in Mumbai slums, 51% in some areas in Pune. The Delhi sero-survey findings published in July 2020 indicate that a whopping 50 lakh people (28%) have already developed 'herd immunity' through 'silent infection', while only 100,000 cases were detected through RT-PCR testing in Delhi (1 in 50). The virus is spreading unevenly with different timelines in different regions. So far, nationwide, 27.6 lakh (0.2% of India's population) cases were detected and around 53,000 died (August 20, 2020).
Perhaps, because of better ‘India-specific’ racial immunity passed on through generations of cellular immunity and ‘memory T cells’, the ‘Case Fatality Rate’ has not been high in India, despite our creaky, rickety and shambolic health care systems. This is a sliver of silver lining for us. Moreover, there is evidence to say that SARS-CoV-2 - specific memory T cells are found in infected persons with or without symptoms -- even in those who did not develop antibodies (seronegative). Memory T cells confer a certain degree of adaptive immunity which may be longer-lasting than that with antibodies.
In addition, the following is the authentic information about it. A recent study of an integrated sequence-based analysis of COVID-19 genomes from different countries yielded interesting findings
The phylogeny of the genomes also makes it evident that a unique mutation in the spike surface glycoprotein (A930V - 2435 C>T) is present in the Indian sequence. Any variation in the immunity or response to treatment may be due to this 'India-specific' difference. COVID-19 genomes, host-virus interaction and pathogenesis may vary from country to country (https://doi.org/10.1101/2020.03.21.001586).
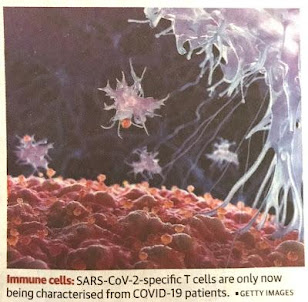
COVID-19-specific Memory T cells
Many people all over the world are exposed to four different coronaviruses that cause 'common cold'. The common cold infections produce what are called 'Memory T cells' or 'Memory CD4 T cells' or 'Memory Helper T cells' or 'pre-existing cross-reactive memory T cells'. These memory T cells may confer some immunity against SARS-CoV-2 also. This is called 'Pre-existing immunity' in individuals who were never exposed to SARS-CoV-2. It may be possible that Indians have more of these cells which reduce the severity and death rate of COVID-19. In one study (La Jolla Institute for Immunology, California) it was found that 28% of healthy blood donors were found to have the pre-existing cross-reactive memory T cells against spike or membrane proteins of SARS-CoV-2. The pre-existing cross-reactive memory T cells might be from previous exposures to common cold coronaviruses. This is an unanticipated degree of 'population-level immunity' against COVID-19. It may be more in the Indian population.
MUTATIONS
The coronavirus keeps changing through mutations. The SARS-CoV-2 that is present in India may not be the same as the one that caused the first case in China. There are at least six identified strains of the virus in circulation across the globe (these are usually referred to as 'strains' or 'mutants', but, they should more appropriately be called 'lineages' or 'clades' or subtypes'). Ten lineages have evolved from the ancestral type --the Wuhan virus type. Based on the revised time-stamped nomenclature, there are now (Aug 2020) 5 lineages -- 19A, 19B, 20A, 20B and 20C. The lineages 20A, 20B and 20C all have the D614G mutation. The D614G lineages have become dominant in India -- 20A in northern and Eastern; 20B in southern and western. The D614G mutant viruses are super-rapid spreaders, but not very lethal. They are very dominant in Europe and North America but not so much in East Asia. They go on mutating. Some are not effective and die out. Some may become more virulent. While the G strain is the most common (which dominated the earlier D strain after March 2020), some have vanished. As in August 2020, a swap between amino acids, identified as D and G, at position 614 in the code of the virus's spike protein produced a variant mutant called D614G which is currently the dominant strain worldwide. The strains present in the US are similar to those in Europe, perhaps due to the travel factor. In India, the first coronavirus was the L strain originating in Wuhan, which eventually mutated into the S and G strains and spread all over the country. Due to closing of borders between States during the lockdown period, different types of mutations might have occurred in different States. The Malaysian case from Tamil Nadu raises the possibility of the D614G strain being in Tamil Nadu. A particular vaccine developed may or may not be very effective against a different mutant. 'An effective vaccine must be against the entire diversity of the virus'. Some say that not giving a vaccine is better than giving a partially effective vaccine. For more about this virus read under the subheading "What is this virus about ?" on this blog below.
2. BCG VACCINATION:
Bacillus Calmette Guerin (BCG) vaccine comprises one kind of live but weakened (attenuated) tuberculosis (TB) bacilli usually given to infants to protect them against some forms (like military and meningeal) of TB. You may be wondering: "What's the connection between BCG and COVID-19 ?" Most surprising is the assumption that BCG vaccination might have protected the countries where BCG vaccination is in general use - protection from COVID-19, though BCG is meant for protection against tuberculosis (TB). The assumption arises out of scientific studies (New York Institute of Technology, USA). In a study (University of Texas, Houston) covering 178 countries, it is found that death rates due to coronavirus are lower by a factor of 10 in countries that had a strong BCG vaccination regimens. It is found that morbidity and mortality due to COVID-19 are high in countries where BCG vaccination is not in practice universally (Spain, Italy, France, USA, etc.). The COVID-19 didn't affect the countries where BCG vaccination is given soon after birth universally since a very long time (India, Japan, etc.). Death rates are low even when infection rates are moderate in Malaysia, Ireland, the Czech Republic, the Slovak Republic, Hungary, Costa Rica, India and many other nations which have strong BCG programmes. All the same, Germany, Norway and Denmark have low death rates though they didn't have BCG cover. Interestingly, within Germany, the former East German part which had a strong BCG regimen has now a lower rate of mortality due to coronavirus. There seems to be good correlation.
What does bacterial TB vaccine have to do with viral COVID-19 ? Most of the Indians had BCG which may confer immunity against many bacteria and viruses. Hence, perhaps, the death rate due to COVID-19 is low in India.
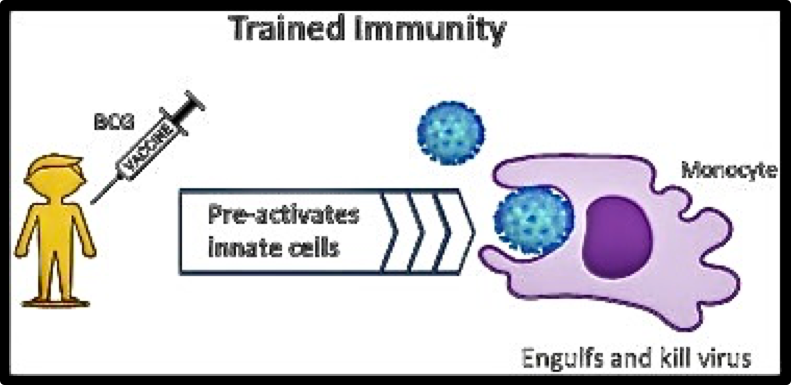
Almost all of us in India were given BCG vaccination (from 1948 onwards) soon after birth to prevent some forms of TB. We seem to be lucky that we may have some immunity against coronavirus also, unexpectedly. BCG vaccination significantly increases the secretion of pro-inflammatory cytokines, specifically IL-1B which has been shown to play a vital role in 'antiviral immunity' - 'trained immunity'. And, BCG vaccination has been reported to offer broad spectrum protection against respiratory infections. Thus, the BCG protection might influence the morbidity and mortality due to COVID-19 by protecting people from co-occurring infections and sepsis which ultimately kill (https://doi.org/co.1101/2020.03.24.20042973).
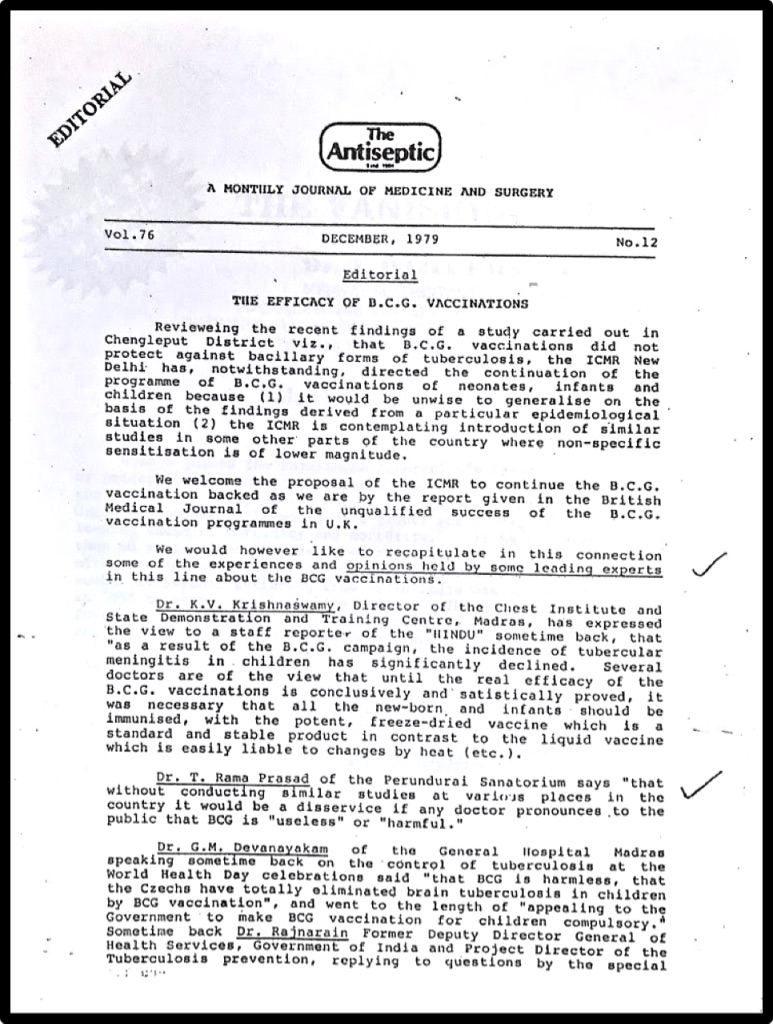
A photocopy of an editorial published 40 years ago in a medical journal wherein my opinion on BCG vaccination was mentioned is attached below.
BCG has been one of the most successful immunotherapies since 1977. It has been in use for bladder cancer. It may also be useful in colorectal cancer, leprosy and Buruli ulcer. It may non-specifically reduce mortality in low-income countries and reduce other health problems including sepsis and respiratory infections, when given early in life. Some are studying its effect on Type 1 diabetes. BCG vaccine is in Phase-3 trials (as of March, 2020) in studies to prevent COVID-19 in health care workers in Australia and the Netherlands. Neither country practises routine BCG vaccination.
All this does not mean that BCG can be used as a vaccine or as a preventive against COVID-19. It only means that this preliminary analysis of data indicates that one of the several factors accountable for the variation of morbidity and mortality among several countries may be the BCG factor. A lot of research is to be conducted before any conclusive evidence can be put forth on this matter.

On July 13, 2020, a BCG study trial is initiated to evaluate the effect of BCG in preventing or modifying COVID-19 in the age group of 60 to 95 years at the National Institute for Research in Tuberculosis (NIRT) at Chetpet, Chennai under the auspices of the Indian Council of Medical Research (ICMR). Five more centres are chosen for this study in Gujarat, Rajasthan, Madhya Pradesh, Maharashtra and Delhi.
3. Subclinical TUBERCULOSIS infection may also act like BCG vaccination. In India, tuberculosis germs are present in the air that is breathed in. In most people they don't cause disease but may increase their immunity. This may be one of the reasons for the low mortality in India due to COVID-19. It should be studied to validate this reasoning.
4. GENETIC FACTORS
There may be individual genetic factors which may influence contracting the disease or the severity of the disease. For example, variants of the gene TLR7 along with defects in the production of immune system molecules of type I and type II interferons may influence immune response, susceptibility to the virus and the vulnerability to 'cytokine storm'.
Now, let us go to 2022 and read the article below :
Rama Prasad. T., BCG and COVID. The Antiseptic, 2022 November, Vol. 119; No. 11; P: 11-19,
Indexed in IndMED – www.antiseptic.in

COVID world: This is one of the 2 dozen articles written in 2 dozen months by a single author (T. Rama Prasad) on a single subject (COVID) and published in a single medical journal (The Antiseptic) -- a WORLD RECORD in Medical Journalism.
The last 17 pages ‘about me’ and my ‘PAY WHAT YOU CAN’ Clinic are not part of the article.
-- Dr. T. Rama Prasad, ‘PAY WHAT YOU CAN’ Clinic, Perundurai, India
---------------------------------------------------------------------------------------------
. BCG and COVID .
RAMA PRASAD T.
Dr. T. Rama Prasad,
Formerly: Medical Superintendent (Special) of RTS & IRT Perundurai Medical College and Research Centre,
Perundurai, Tamil Nadu, India.
Presently: Director of ‘PAY WHAT YOU CAN’ Clinic, Perundurai, Erode District, TN – 638052. drtramaprasad@gmail.com WhatsApp +91 98427 20393 BLOG https://drtramaprasad.blogspot.com
WEBSITE www.rama-scribbles.in Twitter @DrRamaprasadt Facebook T Rama Prasad
Telegram Dr T Rama Prasad
`

A MONTHLY JOURNAL OF MEDICINE AND SURGERYSN
Vol. 119 No. 10 October 2022 ISSN 0003 5998
Indexed in IndMED Email: admin@theantiseptic.in www.theantiseptic.in
BCG and COVID
RAMA PRASAD T.
.
Dr. T. Rama Prasad,
Formerly: Medical Superintendent (Special) of RTS & IRT Perundurai Medical College and Research Centre,
Perundurai, Tamil Nadu. Presently: Director of ‘PAY WHAT YOU CAN’ Clinic, Perundurai, Erode District, TN – 638052.
Specially Contributed to “The Antiseptic” Vol. 119, No. 11
--------------------------------------------------------------------------------------------------------------------------------------------
ABSTRACT
By a strange quirk of immunological twist, BCG has come to play in the ‘centre court’ on a new turf. Nearly three years into the global pandemic, we’re still wondering whether the century-old BCG played a part in the prevention of COVID-19 during the COVID pandemic, and whether it would have a future role to play. The foundation for this thinking comes from a number of articles which suggest a correlation between long-standing national BCG programmes and the morbidity / mortality due to COVID-19. While BCG had been in use in many countries for a very long time to protect children against severe forms of tuberculosis, experimental studies have revealed that BCG can also elicit a ‘non-specific immune response’ against some viral and non-mycobacterial infections. A few of the strange and bewildering aspects of this age-old BCG are highlighted in this article.
Key words: BCG vaccination, Tuberculosis, SARS-CoV-2, COVID-19, Covid-19 pandemic, Non-tuberculous mycobacteria, Trained immunity
---------------------------------------------------------------------------------------------------------------------------------------
Introduction
True to the proverb “Old is Gold”, the century-old ‘Bacillus Calmette-Guerin (BCG)’ vaccine seems to glitter like gold in the COVID (SARS-CoV-2 / COVID-19) era albeit with no robust evidence of its value. Numerous studies are in progress to evaluate its utility in COVID. Its luck can shine if positive evidence ensues. BCG seems, apparently, to have dampened the virulence and pathogenicity of COVID-19 in countries where BCG has been in use ‘universally’. And, BCG seems to have arrived in a new ‘avatar’ in the ongoing ‘drama’ of COVID-19, and may hold a place in future pandemics by virtue of its role as an inducer of ‘trained immunity’.
The urgency and uncertainty in matters connected with COVID prompted researchers to speedily look out for new applications in the old ones. During the COVID pandemic, many drugs had been ‘repurposed’ to prevent or treat COVID-19. Some made a ‘good business’ after which they were abandoned as useless ! Some grandma era’s remedies seemed to work, though such traditional methods seem incongruous in our technical age. Occurrence of infection after being ‘fully vaccinated’ has considerably piqued at the vaccine protagonists. There has been a buzz about the protective effect of BCG vaccine in COVID, based on epidemiological correlations and initiation of ‘randomized control trials (RCTs)’.1, 2, 25, 26
Though the causal relationship isn’t proved, there seems to be a striking correlation between BCG and COVID, indicative of protective attributes of BCG. The ‘non-specific effects (NSEs)’ of the BCG vaccine over the immune system form the basis for the possible utility of BCG vaccine in COVID.1, 2, 25, 26 While the present knowledge and data are insufficient to hope that BCG can be superior to the presently available COVID vaccines, it may be profitable to have a look into the possible broad role of BCG in preventing COVOD-19 and some other diseases as well. A few academic observations and some random thoughts on this subject are briefly mentioned in this article.
“Fight the Big Three”, a historical nugget
A ‘big’ four-page EDITORIAL titled “Fight the Big Three” was published in The Antiseptic on August 15, 1945, six days after the conclusion of World War II. The editorial of the premier journal which was established in 1904 stated that tuberculosis, leprosy and cancer were the three most dangerous scourges that ravaged India, and that the war against tuberculosis was no less important or damaging than the war against militarist Japan (Editorial, “Fight the Big Three,” The Antiseptic 42, no. 8 (1945): 457–60. ).3 This issue of The Antiseptic was published when I was a three-year-old toddler (I am now 80-years-young !). Age is partly a psychological factor – my article titled ‘You are not old’ may be accessed at: https://drtramaprasad.blogspot.com/2017/04/you-are-not-old_30.html .4 This is by the way. Ironically, now, after about eight decades, the editorial comment still holds good, with 1.5 million people being killed by tuberculosis (TB) and 10 million by cancer, every year worldwide now.
The historically controversial BCG
Mired in controversies since its birth a century ago, BCG remains a controversy even today. Leaving the remote past, in 1950s when mass BCG campaigns were launched by the ‘International Tuberculosis campaign’ and the World Health Organization (WHO), BCG was met with fierce resistance by researchers and the public as well, deploying scientific disagreements, in many countries, on its safety and efficacy. In India, A. V. Raman through his articles in ‘People’s Health’ and C. Rajagopalachari / Rajaji (the last Governor–General of India and the former Chief Minister of Madras State) through his ‘anti-BCG pamphlets’ marshalled vehement arguments against BCG, even citing articles published in The Lancet and the Journal of the American Medical Association.5, 6
In those days, there was a cleavage in international health system – a disagreement between the WHO and the UNICEF over mass BCG campaigns – and scientific bodies which was adroitly exploited by Raman and Rajaji. Further, Raman said that the ulterior motive of BCG campaigns was to use Indians as guinea pigs, and Rajaji fanned the flames highlighting his conviction of children falling ill and dying due to BCG. They were not alone. There were many ‘Ramans’ and ‘Rajajis’ in other countries too who spearheaded anti-BCG campaigns.
The common denomination underlying the BCG controversy and the TB control in postcolonial India and Southeast Asia during the 1950s was the notion of fractured sovereignties. BCG was the political trope of post-World War II reconstruction in ‘British India’. Whether it’s right or wrong, it’s human – in this day and age, are we not having fiercely agitating ‘antivaxxers’ against Covid vaccines ? Control of diseases has become a fool’s errand with ramifications of geopolitics without geo-economics. It’s an allegorical story for the anthology.
Today’s (October 7, 2022) news of the shameful tragedy of the death of 66 children in The Gambia of West Africa, allegedly due to adulterated cough syrups, brings to memory the ‘Lubeck disaster’ of 1930s when 72 children died due to BCG vaccination with a virulent strain in Lubeck of northern Germany. The disaster cast a shadow over the safety of BCG for a very long time. We don’t yet know how long the shadow would be on Indian pharmaceutical industry, as the cough syrups are reported to be made in India. The trade is getting murkier by the day.
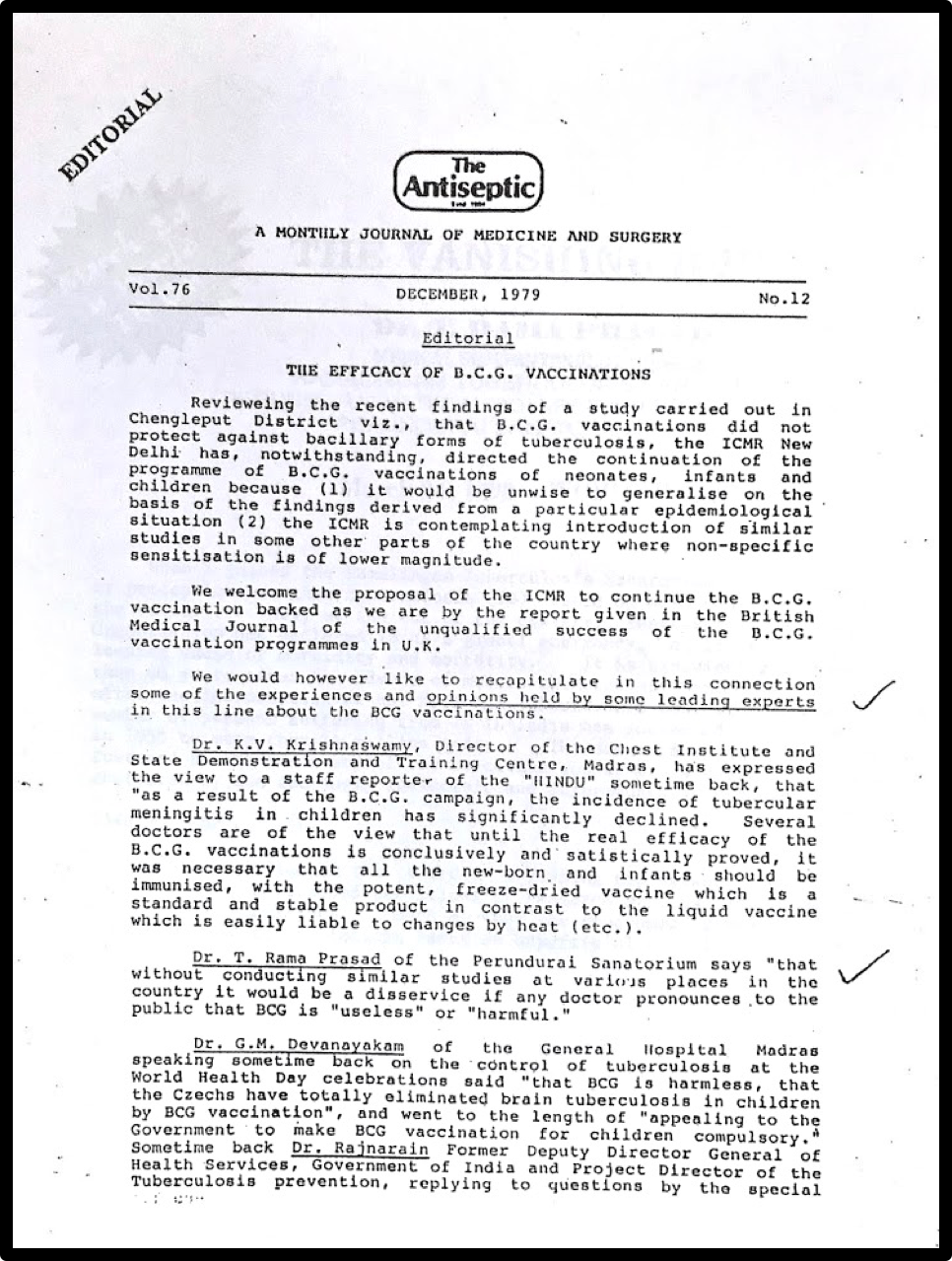
Scenario 40 years ago
Even in the relatively recent past (more than 40 years ago, in 1979), there was a raging controversy about giving BCG vaccine in India, in view of a ‘robust’ study which found BCG not to be beneficial in protecting against TB (ICMR BCG Trial in Chingleput district).14 At that point of time, in the context of the interim ‘negative’ results of the study and the raging controversy about continuing BCG, the premium medical journal, The Antiseptic wrote an editorial mentioning opinions of some leading experts in the field (including me) who supported continuance of BCG. In the editorial, the journal mentioned my view as: “Dr. T. Rama Prasad of the Perundurai Sanatorium says ‘that without conducting similar studies at various places in the country it would be a disservice if any doctor pronounces to the public that BCG is ‘useless’ or ‘harmful’.” (Editorial, “THE EFFICACY OF B.C.G. VACCINATIONS” The Antiseptic, December 1979, Vol.76, No. 12). 7
BCG and children, 4 decades ago
And, in my article titled ‘CHILDHOOD TUBERCULOSIS’ published in The Antiseptic of August and September (Part I & II) of 1979, I mentioned: “ … There has been a raging controversy all over the world about the efficacy of BCG in preventing tuberculosis. … It would be a pity if the drive to vaccinate the eligible population gets bogged down in the mire of controversies. Though the opinion on the efficacy of BCG seems to be divided, there is now a general agreement that it is not harmful. So long as incontrovertible evidence is lacking to conclude that BCG is ineffective, prudence demands that we, in India, should not spare any effort to give potent ‘freeze-dried’ BCG vaccination to as many eligible children as possible. It is preferable to vaccinate a child after the age of one year, if the child comes from the higher socio-economic class wherein the chances for the infant to be exposed to the infection are low. In the low socio-economic class, the vaccination is to be done soon after birth. …”.8
UPDATE: The final results of the famous and truly monumental 15-year ICMR BCG Trial in Chingleput district (1968 to 1983, with 281,161 persons of the age of one month or above) led to the conclusion that BCG offers no protection against ‘adult type’ of bacillary TB.14 However, some other studies found BCG to be highly effective in protecting children from ‘progressive primary (non-pulmonary) TB’, particularly ‘TB meningitis’ and ‘miliary TB’. It is perplexing and confounding to note that even four decades after the publication of my article cited above, the BCG scenario is more or less unchanged, and even more challenging. With the advent of COVID, BCG is once again in the spotlight. It is known that children are better protected from COVID than adults. This may be due to the BCG given at birth which may protect up to adulthood, or it may be because the ‘immune dysfunction and cytokine production’ are much less in children compared to adults.
Swift academic reaction
COVID upended the world and reversed many things. People were searching for an ‘alternative Covid-free universe’ ! With ambiguity abounding, researchers swiftly swung into action to evaluate BCG in relation to COVID. The subject gained so much relevance, with a sudden stimulus, that as many as twenty BCG study trials were already in various clinical stages even as early as January 2021, and many more entered the pipeline since then. Clinical trials are going on in the Netherlands, Australia, the UK, Germany and India to evaluate the efficacy of BCG in COVID. The results available until now (October 2022) are extremely mixed.
One study claims a link between low Covid impact and wide BCG coverage, another dismisses the evidence as flimsy and floppy. One study over a period of 15 months did show positive results in prevention of COVID in BCG-naïve people with ‘Type 1 diabetes’.9 On the other hand, revaccinating with BCG didn’t prevent COVID infection in healthcare workers over a period of five months.10 It would, of course, take a long time to make a meaningful meta-analysis on the subject to draw any valid and robust conclusions. Research in COVID gained more traction as the existing vaccines and medicaments like plasma therapy, tocilizumab, monoclonal antibodies, remdesivir, etc. didn’t live up to our expectations.
Why BCG now ?
Spectacular advancements are made in well-developed countries. Infrascan, a pocket-sized CT scan gadget is made available in the US in September 2022. PUMP is another pocket-sized gadget, made by the US-based Unitree Robotic company, which may replace a gym. Next to the ‘mRNA’ vaccine, ‘MVA/S’ vaccine, ‘receptor-binding domain-dimer-based’ vaccine and a ‘plant-based coronavirus-like particle’ vaccine are the buzzwords in vaccinology.11 That being the situation, ‘why BCG now ?’ What’s the wisdom ? The verdict is still up in the air.
In this day and age, research on BCG to mitigate COVID may seem to be an old-fashioned academic pastime. This goes against the grain of ‘Big Pharma’ thinking. But, the flipside is that modern medical methods couldn’t prevent the one million ‘Covid deaths’ in the US out of a population of just 0.3 billion while there were only half that number of deaths in India with a huge population of 1.4 billion with a comparatively poor health infrastructure. Most of the people in India had BCG vaccination while almost none had it in the US. During the Covid pandemic, most in India looked for old systems of medicine while many medicines of ‘modern medicine’ were approved and soon later dropped. Most in India have old lifestyle habits while the modern western lifestyle had been blamed for the onset of the pandemic.
The afterglow of the COVID vaccines was a tad dimmed by the Omicron, with numerous ‘breakthrough’ infections, and it is a given that the pandemic is fading now more due to the ‘natural immunity’ gained. We should not remiss the hypothesis that COVID didn’t do much harm in countries of unhealthy environment with a huge load of ‘subclinical infections’ by various microbes, unlike in the highly hygienic and highly developed countries. And, it is to be noted that the less privileged countries had a ‘universal’ BCG programme mostly. All this makes one tempted to study the old ones, including BCG.
Is it BCG or other infections that protect ?
During the COVID pandemic, a concept that BCG could confer protection against COVID has emerged. The foundation for this concept comes from several articles, including the one by Miller et al., which suggest a correlation between countries with a long history of BCG vaccination and the morbidity / mortality due to COVID.12 Proportionately less cases, milder illness and a lower death rate in BCG-vaccinated populations as compared to BCG-non-vaccinated populations across countries and hemispheres was observed.13 However, some opined that the evidence is not strong. On the flipside of the evidence, the BCG given to children at birth could not have protected adults and the aged as it has presumably a short duration of protection of less than 20 years. As such, in those ‘BCG-protected’ countries, some other factors might be playing a role – like endemic infections such as dengue, chikungunya, malaria and other tropical infections, and ‘environmental non-tuberculous mycobacteria (NTM)’ of around 150 species. These infections, especially the NTM , may protect through various interferons, induction of immunological memory-eliciting-lymphocytes response, trained immunity, elevation of innate and adaptive immunity, etc. Hence, the people in these countries might have had NTM infections (mostly not experiencing symptoms), and numerous other infections which could have enhanced ‘native immunity’.
How BCG may protect ?
Experimental studies indicate that BCG can elicit a ‘non-specific immune response’ against several viral and non-mycobacterial infections. BCG is believed to have what are called ‘nonspecific effects (NSEs)’ which are immune responses having the capacity to protect against infections other than tuberculosis. These effects may be due to the ‘immunological memory-eliciting-lymphocytes’ and ‘trained immunity’. These responses may be mediated by ‘heterologous lymphocyte response’ and the initiation of ‘innate immune memory’ which is likely to be applicable to SARS-CoV-2. BCG vaccination is also known to induce enhanced frequencies of ‘memory T and B cells’ and ‘dendritic cell subsets’ in elderly people. In addition, ‘environmental mycobacteria (NTM)’, through their ‘subclinical infections’ might have conferred immunity, akin to the one induced by vaccines, to protect against severity and deaths due to COVID. In this context, research on developing a more ‘broad-spectrum BCG’ vaccine is to be encouraged.
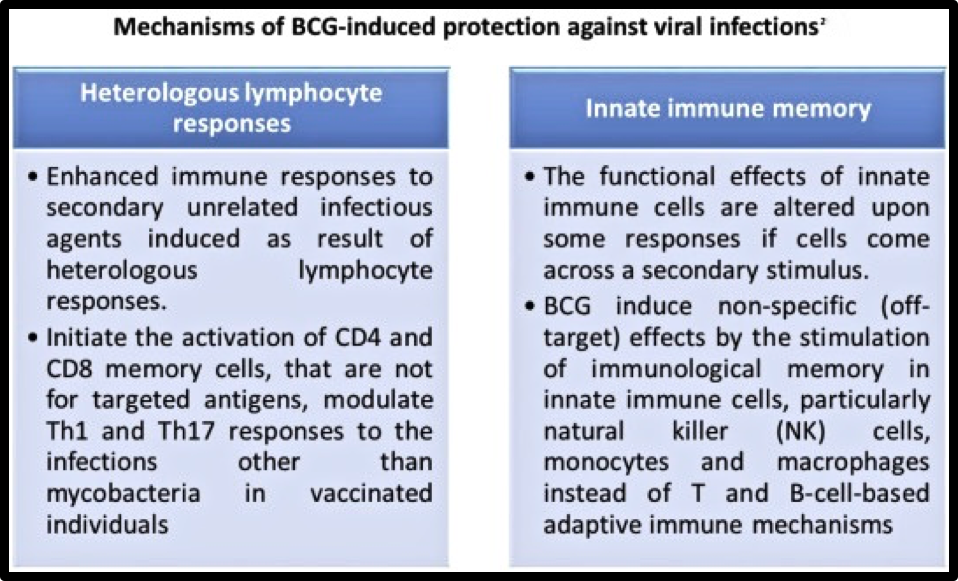
Non-specific effects (NSEs) of BCG
BCG vaccine is characteristic of enhancing immune responses through what is popularly known as ‘trained immunity’ which offers protection against a variety of pathogens / diseases like Salmonella, Shigella, malaria, respiratory viruses, etc. other than Mycobacterium tuberculosis. The ‘trained immunity’ is the basis for using BCG as an immunotherapy agent in bladder cancer, malignant melanoma, etc. The ‘trained immunity’ is the enhancing response mediated through the non-specific effects (NSEs) of BCG over the immune system. The NSEs are mainly mediated by potentiating innate immune response through epigenetic mechanisms. The ability to induce potent non-specific immunity is the so-called ‘off-target’ protection against bacterial and viral pathogens. The epigenetic changes within the innate cells act as de novo enhancers to boost the immune response against a secondary challenge.2 By virtue of the NSEs, BCG vaccine decreases all-cause mortality in children. This non-specific effect may be mostly short-lived, though a few observational studies suggest that the NSEs may last till adulthood, even up to the age of 50 years. The efficacy to protect against many infections can be linked to the response of the ‘immunological memory-eliciting-lymphocytes’ and ‘trained immunity’. Unfortunately, BCG can’t protect all forms of TB in all age groups. But, several studies indicate that BCG reduces respiratory tract infections and the risk of pneumonia. A ray of hope comes through the development of a ‘recombinant BCG vaccine’.
Recombinant BCG vaccine
A new BCG-based vaccine called ‘Recombinant BCG vaccine’ is developed. Christened ‘VPM1002’, it is in the pipeline at the Pune-based ‘Serum Institute of India Limited’ under license from the Max Planck Institute for Infection Biology, Berlin and the Vakzine Projekt Management GmbH, Hanover, Germany. It contains a gene which makes it easier for the vaccine to be better recognised by cells of the immune system and which facilitates induction of broader cellular immunity. This new vaccine may be given to HIV-positive babies also unlike the older one which may produce BCG-related TB. The new vaccine which comes after a century of waiting may tackle the difficult Mycobacterium tuberculosis that expresses some 3,000 different antigens. Hence, it is hoped that this vaccine would protect all age groups against drug-sensitive and drug-resistant TB. ‘Recombinant BCG vaccines’ may offer robust protection against COVID-19 through ‘trained immunity’ induced by rBCG along with SARS-CoV-2 specific immune response. They have excellent safety profile, low production cost and good thermal stability (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7386780/ ).24 By extension of the hope, and by a fortunate stroke of serendipity, the ‘recombinant BCG vaccine’ may induce excellent immunity against COVID also – a double delight. Another vaccine, ‘MIP’ (Mycobacterium indicus pranii) is being studied.
A hypothesis
There is a voluminous literature on the association / correlation between BCG and COVID. One may be tempted to draw hasty conclusions from the studies. For a critical appraisal, one has to take into the factors and variables like the differences in testing strategies, reporting bias, demographics, genetic differences in the populations and the strains cultured in the laboratories, health infrastructure, mitigation efforts, a country’s ability to respond to the pandemic, prevalence of comorbidities, population density, environment, ambient temperature, humidity, cultural norms, national policies on BCG vaccination, and the prevailing different phases of the pandemic across various countries.
Results must be interpreted carefully, and the causal relationship should be tested through well-designed clinical trials and appropriately planned studies. Also, the NSEs of the BCG have not been well-studied. The results of the ongoing RCTs may shed some light on the subject. Until then, the association between BCG and COVID may be considered as a hypothesis, and a recommendation to vaccinate with BCG for the prevention of COVID should be reserved.
BCG
Bacillus calmette-Guerin vaccine (BCG), also known as Vaccin Bilie de Calmette et Guerin vaccine and Bacille de Calmette et Guerin vaccine, (all named after Albert Calmette and Camille Guerin) is primarily used to prevent miliary and meningeal TB in children. It is a live attenuated strain derived from Mycobacterium bovis which is also used against Leprosy, Buruli ulcer and other non-tuberculous mycobacterial infections. Additionally, it is found to be useful in treating bladder and colo-rectal cancer. Many countries with a high burden of TB / Leprosy have been using BCG vaccine routinely (‘universal’) whereas some countries like the US and Netherlands had never used it routinely. BCG is on the WHO’s ‘List of Essential Medicines’, and is being given to about 100 million children per year globally.
Unfortunately, BCG is found to be having a widely variable efficacy in different clinical trials, but it remained as the only vaccine against TB over the past 100 years (and counting) since it was first used medically in 1921. A limited rollout started in India in 1948. The reasons for variable efficacy have been discussed at length in a WHO document on BCG.15 Populations living away from the equator like the UK, Norway, Sweden and Denmark seem to have more benefit from BCG compared to those in tropical countries like India, Kenya and Malawi.16, 17 Though the duration of protection by the BCG vaccination is not clear, BCG may have a beneficial effect in preventing various non-tuberculous infections including COVID. Tentative evidence exists for a beneficial ‘non-specific effect’ of BCG vaccination on overall mortality and morbidity in low-income countries.18
‘COVID-TB’, the double whammy
Covid and TB have such significant ‘syndemic’ characters that the two coinfections may be referred to by the term “COVID-TB”. TB used to cause “slow death”, but now onwards the “COVID-TB” may cause “fast-slow” death ! And again, to take a leaf out of our democratic book, they have realised the power of unity ! Clinical trials of evaluating efficacy of BCG against COVID have come in the backdrop of studies which indicated a slower spread of COVID in countries where BCG vaccination to children is given routinely. There are two main diseases of concern for death due to infection in the world at present – COVID and TB.
In early 2020, when the disastrous and devastating COVID was spreading like wildfire, we didn’t have an inkling of its deadly association with the smouldering scourge, TB. Now, it is known that the coinfection of COVID in TB patients had accelerated both the diseases, leading even to deaths. A parallel epidemic of TB may add fuel to the fire. It is not yet clear as to how exactly this happens. This is a dangerous grey area which is to be navigated with utmost caution as the two diseases seem to be mutually aggravating. And, I mentioned the following in my article titled ‘COVID and TUBERCULOSIS’ which was published in The Antiseptic of December 2021 : “ … According to the Centers for Disease Control and Prevention of the US, TB patients are at a greater risk for severe forms of COVID-19. COVID-19 coinfection in TB patients was found to accelerate the disease course of both the diseases which may lead to death. …” 19
TB, the great killer
In 1960s, I thought that we would be talking about TB in 2000s in the same manner that we speak now of telegrams and STD calls, both of which are no longer in our lives now. Intriguingly, now, TB is the leading cause of death worldwide from a single infectious agent. The worst among the endemic diseases is TB, killing 1.5 million people every year globally. In India alone, according to a latest estimate, 1,400 persons die every day due to TB, despite the existence of a ‘National TB Control Programme’ since 1962. This is just another typical example of an outcome of bureaucrats and medical advisors being jointly at work. Or, rather, not at work !
The century-old BCG couldn’t contain the dreaded scourge which seems to be invincible, with 10 million people developing TB every year globally. And, India has a share of 25% in the cases and deaths ! I wrote the following in a special article published in The Hindu of March 15, 2020 (just at the beginning of the COVID pandemic when on March 16, 2022 only five ‘Covid deaths’ were reported) : “ … TB is killing more people than ever before in history — 1,000 people every day in India, at present. This chronic mortality does not become news, whereas one case of COVID-19 grabs the headlines. …” (https://www.thehindu.com/opinion/open-page/a-bad-patch/article31069356.ece ).20, 21
We could not satisfactorily control TB (unlike the other historically dreaded diseases like smallpox, leprosy, plague and cholera) though we had specific drugs to treat; we could not control Covid due to lack of specific drugs (Molnupiravir and Paxlovid are still being studied). The impact of COVID on TB problem (which could not be controlled yet, and riddled with problems of drug-resistance) may become humongous in the long term even as COVID may be contained in the near future, for the simple reason that effective vaccines are being made for COVID while none exists against TB in adults (BCG vaccine protects only to some extent against development of some forms of TB in children – perhaps, it reduced TB infection by about 20% and reduced progression to TB in the infected by about 50%).
It is unfortunate that an effective vaccine against TB (caused by a well-studied Mycobacterium tuberculosis bacterium) couldn’t be developed though the disease has been with the humanity for a very long time – it can be traced to the prehistoric ages (the remains of Pleistocene bison in Wyoming gives evidence of presence of TB over 17,000 years ago). And the cause for the disease was identified around one-and-a-half centuries ago (Robert Koch announced the discovery of the causative bacillus on March 24, 1882). In stark contrast, the expected time of 10 years to produce a vaccine for a coronavirus is ‘compressed’ into 10 months in the case of Covid !3 It would be a fortunate stroke of serendipity if a new recombinant BCG vaccine could be made which blocks both TB and COVID.
When I entered the speciality of TB and Respiratory Diseases, more than half-a-century ago, TB was mostly curable. Now, in spite of availability of newer drugs, cure for TB is more uncertain, due to ‘drug resistance’. My article published in The Hindu of March 15, 2020 highlights this strange phenomenon: https://www.thehindu.com/opinion/open-page/a-bad-patch/article31069356.ece .20
Vicious partners
A scientific study has evaluated the correlation of host-expression with SARS-CoV-2 and interaction of 26 proteins of SARS-CoV-2 with 332 human proteins.22 It was found that Mycobacterium tuberculosis that causes TB shares most of the host protein interaction partners (same interactome) with SARS-CoV-2 which is of utmost importance as both the infections have high affinity towards lung tissues. Lung is commonly involved in most of the cases of COVID and TB. Both the pathogens may induce immunomodulation disorders leading to an unbalanced inflammatory response which can worsen the course of both the diseases.
We still do not know whether manifestations of COVID and TB are directly due to the pathogens or a dysregulated immune system. The pulmonary alveoli are like the battleground for both COVID and TB though TB surreptitiously affects the lungs without alerting immune systems much, while COVID aggressively promotes immunopathology and damages tissues through pyroptosis. The long-term trajectory of these effects remains unknown, as does the probability of success of interventions to subdue the problem. This combo may severely affect ‘high-TB-burden’ countries in Africa, South America and Southeast Asia. This is akin to the association of TB with the ‘human immunodeficiency virus’ (HIV) which resulted in a deadly syndemic of global proportions in the mid-20th century. SARS-CoV-2 infection is also seen as a nosocomial infection in TB cases.
Information explosion
Since the onset of the COVID pandemic, there has been an exponential growth of information on COVID and the related subjects, but the picture is still hazy. Month to month, the scenario has been changing, older concepts being discarded and new ones installed.27 to 64 This can be seen in my two dozen articles over two years on COVID published in The Antiseptic – a world record in medical journalism.27 to 51 Notwithstanding, because of confusing and confounding information, people have questions which have no convincing answers. Some of the tricky questions may be found in my ‘Web Special Premium’ article titled ‘COVID questions’ published in The Hindu of August 28, 2022 ( https://www.thehindu.com/opinion/open-page/covid-questions/article65803119.ece ).23 The article indicates the high level of ‘Covid knowledge’ acquired by the public during the pandemic. There has been an enormous interest in the people to look into technical literature on COVID through social media – this has been the case with my articles cited above.
Stepmotherly treatment
TB seems to be a poor country’s disease while COVID is that of the rich. The rich world seems not to be kind to the BCG of the poor who suffer more from TB, but it has been generous to Covid vaccines of the rich who suffered more from COVID-19. And, there is ‘gold, glitter and glamour’ in Covid research ! For ‘Research & Development’ of Covid vaccines, 8.5 billion US dollars were earmarked (Global Contributions to ACT-Accelerator, Vaccine Category), whereas for TB the amount was a paltry sum of 0.117 billion dollars (Global Funding for TB Vaccine Research). Within two years, more than 20 Covid vaccines received emergency use authorization and about a hundred are in clinical trials, racing against time. For TB, a single vaccine of low efficacy has been in use for the last 100 years and only about 20 are in clinical trials. COVID killed 1.4 million people in a year in its ‘short duration drama’ of a few years, whereas TB has been killing 1.4 million people every year over innumerable number of years. This is a glaring spectacle of inequality in the support by political, financial and pharmaceutical institutions. Should we call it a ‘racial discrimination’ !!!
The reality
The ongoing studies may prove that the ‘Old is Gold’ or that the ‘Old is just a Fossil’. Whatever be the results, we have to look beyond the narrow techno-centric approach that focusses on targeted interventions such as vaccinations, and pursue a holistic approach that correlates disease to lifestyle, thinking and, of course, poverty. Déjà vu ! We need to mind the social, behavioural and economic underpinnings of the diseases, grounding them in logic. ‘Recombinant BCG vaccine’ may be more perfect in doing the job. Perfection is an illusion and non-existent. After mailing this article, I would feel that this article is not written to perfection. That was the case with all the hundreds of my writings.
“Have no fear of perfection – you’ll never reach it.” -- Salvador Dali
We are no fettle to be ecstatic about the current declining trend of COVID or the good old ‘Pushpaka Vimanam’ and ‘Aryabatta’, about whom we are rightly proud of. It’s not just the question of finding a new vaccine. We have to be ready to face new microbes. The painful hardships experienced in 2020-21 infused terror into all humans – princes in palaces to paupers on pavements; officegoers to homemakers; bosses to servants; children to adults; employers to employees – due to the rational and irrational regulations; real and imaginary sufferings. Fear, fear and fear ! Fear is infused during childhood to protect us. The fear goes on growing as we grow older and older in these distressing times of COVID.
If something worse than the Delta (whose world tour started in India) evolves, the world would – Heaven forbid -- be back to the drawing board.
REFERENCES
World Health Organization. Bacille Calmette-Guérin (BCG) vaccination and COVID-19. Available from: https:/ /www.who.int/news-room/commentaries/detail/ bacille- calmette-guérin-(bcg)-vaccination-and-covid-19.
SAGE Working Group on BCG Vaccines and WHO Secretariat. Report on BCG vaccine use for protection against mycobacterial infections including tuberculosis, leprosy, and other nontuberculous mycobacteria (NTM) infections. World Health Organization; 2017. Available from: https://www.who.int/immunization/sage/ meetings/ 2017/october/1_BCG_report_revised_version_online.pdf. Accessed April 14, 2020.
Editorial, “Fight the Big Three,” The Antiseptic 42, no. 8 (1945): 457–60.
https://drtramaprasad.blogspot.com/2017/04/you-are-not-old_30.html
C. Rajagopalachari, BCG Vaccination: Why I Oppose It (Madras: Jupiter Press, 1955), 7, Accession No. 109290, Roja Muthiah Research Library.
A.V. Raman, “Editorial,” People’s Health 4, no.4 (1950): 177–80.
Editorial, “THE EFFICACY OF B.C.G. VACCINATIONS” The Antiseptic, December 1979, Vol.76, No. 12
Rama Prasad, T., CHILDHOOD TUBERCULOSIS. The Antiseptic, 1979 August and September (Part I & II).
Faustman, Denise L.; Lee, Amanda; Hostetter, Emma R.; Aristarkhova, Anna; Ng, Nathan C.; Shpilsky, Gabriella F.; Tran, Lisa; Wolfe, Grace; Takahashi, Hiroyuki; Dias, Hans F.; Braley, Joan; Zheng, Hui; Schoenfeld, David A.; Kühtreiber, Willem M. (September 2022). "Multiple BCG vaccinations for the prevention of COVID-19 and other infectious diseases in type 1 diabetes". Cell Reports Medicine. 3 (9): 100728. doi:10.1016/j.xcrm.2022.100728.
Upton, Caryn M.; van Wijk, Rob C.; Mockeliunas, Laurynas; Simonsson, Ulrika S.H.; McHarry, Kirsten; van den Hoogen, Gerben; Muller, Chantal; von Delft, Arne; van der Westhuizen, Helene-Mari; van Crevel, Reinout; Walzl, Gerhard; Baptista, Pedro M.; Peter, Jonathan; Diacon, Andreas H. (June 2022). "Safety and efficacy of BCG re-vaccination in relation to COVID-19 morbidity in healthcare workers: A double-blind, randomised, controlled, phase 3 trial". eClinicalMedicine. 48: 101414. doi:10.1016/j.eclinm.2022.101414.
Rama Prasad. T., COVID medical literature – the Good, the Bad and the Ugly. The Antiseptic, 2022 September; Vol. 119; No. 9; P: 07-19; Indexed in IndMED – www.antiseptic.in
Br Med J (Clin Res Ed), 288 (6416) (1984), p. 564
Allergy, 75 (7) (2020), pp. 1824-1827
Tuberculosis Research Centre (ICMR), Chennai, Fifteen-year follow up of trial of BCG vaccine in south India for tuberculosis prevention. Indian J Med Res 1999; 110: 56-69.
Fine PE, Carneiro IA, Milstein JB, Clements CJ (1999). "Chapter 8: Reasons for variable efficacy" (PDF). Issues relating to the use of BCG in immunization programmes: a discussion document (Report). Geneva, Switzerland: World Health Organization. hdl:10665/66120. WHO/V&B/99.23.
Colditz GA, Brewer TF, Berkey CS, Wilson ME, Burdick E, Fineberg HV, Mosteller F (March 1994). "Efficacy of BCG vaccine in the prevention of tuberculosis. Meta-analysis of the published literature". JAMA. 271 (9): 698–702. doi:10.1001/jama.1994.03510330076038. PMID 8309034.
Jump up to: a b Fine PE (November 1995). "Variation in protection by BCG: implications of and for heterologous immunity". Lancet. 346 (8986): 1339–45. doi:10.1016/S0140-6736(95)92348-9. PMID 7475776. S2CID 44737409
Biering-Sørensen S, Aaby P, Napirna BM, Roth A, Ravn H, Rodrigues A, et al. (March 2012). "Small randomized trial among low-birth-weight children receiving bacillus Calmette–Guérin vaccination at first health center contact". The Pediatric Infectious Disease Journal. 31 (3): 306–8. doi:10.1097/inf.0b013e3182458289. PMID 22189537. S2CID 1240058.
Rama Prasad, T., COVID and Tuberculosis. The Antiseptic, 2021 December; Vol. 118; No.12; P: 11-17; Indexed in IndMED
https://www.thehindu.com/opinion/open-page/a-bad-patch/article31069356.ece
https://drtramaprasad.blogspot.com/2017/04/tuberculosis-in-india_29.html
https://www.thehindu.com/opinion/open-page/covid-questions/article65803119.ece
Jump up to: a b Fine PE (November 1995). "Variation in protection by BCG: implications of and for heterologous immunity". Lancet. 346 (8986): 1339–45. doi:10.1016/S0140-6736(95)92348-9. PMID 7475776. S2CID 44737409.
Colditz GA, Brewer TF, Berkey CS, Wilson ME, Burdick E, Fineberg HV, Mosteller F (March 1994). "Efficacy of BCG vaccine in the prevention of tuberculosis. Meta-analysis of the published literature". JAMA. 271 (9): 698–702. doi:10.1001/jama.1994.03510330076038. PMID 8309034.
Rama Prasad. T., The Long COVID. The Antiseptic, 2022 October; Vol. 119; No. 10; P: 12-19; Indexed in IndMED – www.antiseptic.in
Rama Prasad. T., COVID medical literature – the Good, the Bad and the Ugly. The Antiseptic, 2022 September; Vol. 119; No. 9; P: 07-19; Indexed in IndMED – www.antiseptic.in
Rama Prasad. T., Origin of COVID. The Antiseptic, 2022 August; Vol. 119; No. 8; P: 09-17; Indexed in IndMED – www.antiseptic.in
Rama Prasad. T., COVID Deaths. The Antiseptic, 2022 July; Vol. 119; No. 7; P: 14-22; Indexed in IndMED – www.antiseptic.in
Rama Prasad. T., The long and the short of COVID in India. The Antiseptic, 2022 June; Vol. 119; No. 6; P: 14-27; Indexed in IndMED – www.antiseptic.in
Rama Prasad. T., COVID Fear and Paranoia. The Antiseptic, 2022 May; Vol. 119; No. 5; P: 09-17; Indexed in IndMED – www.antiseptic.in
Rama Prasad, T., Post-OMICRON Peregrination. The Antiseptic, 2022 April; Vol. 119; No. 4; P: 06-14; Indexed in IndMED – www.antiseptic.in
Rama Prasad, T., COVID – still an enigma. The Antiseptic, 2022 March; Vol. 119; No. 3; P: 20-25; Indexed in IndMED -- www.antiseptic.in
Rama Prasad, T., OMICRON – A Paper Tiger. The Antiseptic, 2022 February; Vol. 119; No. 2; P:12-21; Indexed in IndMED – www.antiseptic.in
Rama Prasad, T., Ominous Omicron of COVID. The Antiseptic, 2022 January; Vol. 119; No. 1; P:25 – 29; Indexed in IndMED – www.antiseptic.in
Rama Prasad, T., COVID and Tuberculosis. The Antiseptic, 2021 December; Vol. 118; No.12; P: 11-17; Indexed in IndMED -- www.antiseptic.in
Rama Prasad, T. The Science and Nonsense around COVID. The Antiseptic, 2021 November; Vol. 118; No. 11; P: 8-14; Indexed in IndMED -- www.antiseptic.in
Rama Prasad, T. COVID, Children and Schools. The Antiseptic. 2021 October; Vol.118; No.10; P: 08-18; Indexed in IndMED -- www.antiseptic.in
Rama Prasad, T. India’s Third COVID Wave. The Antiseptic. 2021 September; Vol.118; No.9; P: 14-20; Indexed in IndMED – www.antiseptic.in
Rama Prasad, T. Vagaries of India’s COVID Vaccination Policy. The Antiseptic. 2021 August; Vol.118; No.8; P: 10-16; Indexed in IndMED – www.antiseptic.in
Rama Prasad, T. Mucormycosis and COVID-19 in India. The Antiseptic. 2021 July; Vol.118; No.7; P: 21-26; Indexed in IndMED -- www.antiseptic.in
Rama Prasad, T. Disastrous Second COVID Wave in India. The Antiseptic. 2021 June; Vol.118; No.6; P: 20-27; Indexed in IndMED – www.antiseptic.in
Rama Prasad, T. COVID Variants. The Antiseptic. 2021 May; Vol.118; No.5; P: 11-14; Indexed in IndMED -- www.theantiseptic.in
Rama Prasad, T. Covishield or Covaxin ? The Antiseptic. 2021 April; Vol. 118; No. 4; P: 12-16; Indexed in IndMED – www.theantiseptic.in
Rama Prasad, T., Versha Rajeev. The Conundrum of COVID-19 Vaccines. The Antiseptic. 2021 January; Vol.118; No.1; P: 10-17; Indexed in IndMED – www.theantiseptic.in
Rama Prasad, T. 40+15 Hypoxia Test in COVID-19. The Antiseptic. 2020 December; Vol. 117; No. 12; P: 13-17; Indexed in IndMED – www.antiseptic.in
Rama Prasad, T., Versha Rajeev. Antiseptics, Disinfectants and COVID-19. The Antiseptic. 2020 November; Vol.117; No.11; P: 26-28; Indexed in IndMED – www.antiseptic.in
Versha Rajeev., Rama Prasad, T. Fear and COVID. Health. 2020 November; Vol.98; No.11; P:31-32
Rama Prasad, T., Versha Rajeev. Tea and COVID. Health. 2020 October; Vol.98; No.10; P: 4-6.
Rama Prasad, T. Is the “Lockdown Medicine” too toxic ? The Antiseptic. 2020 October; Vol. 117; No. 10; P: 13-15; Indexed in IndMED – www.theantiseptic.in
Rama Prasad, T., Digital clubbing and Hypertrophic Pulmonary Osteoarthropathy. The Antiseptic, 1979 April, Vol. 76; P: 213-215
https://drtramaprasad.blogspot.com/2017/04/tuberculosis-in-india_29.html
https://drtramaprasad.blogspot.com/2020/06/coronavirus-covid-19-sars-cov-2_43.html
Rama Prasad, T., Versha Rajeev. https://drtramaprasad.blogspot.com/2017/04/covid-crocodiles.html
https://drtramaprasad.blogspot.com/2017/04/hydroxychloroquine-hcq-and-coronavirus_29.html
https://drtramaprasad.blogspot.com/2017/04/corona-and-charles-darwin.html
https://drtramaprasad.blogspot.com/2017/04/modern-medicine-good-bad-and-ugly_30.html
https://drtramaprasad.blogspot.com/2017/04/yellow-nail-syndrome_28.html
https://journal.chestnet.org/article/S0012-3692(16)40458-7/fulltext
http://drtramaprasad.blogspot.com/2017/04/what-you-can-clinic_30.html
https://www.thehindu.com/opinion/open-page/a-bad-patch/article31069356.ece
https://www.thehindu.com/opinion/open-page/covid-questions/article65803119.ece
OPEN PAGE -- THE HINDU, August 28, 2022 -- A ‘Web Special Premium Article’
COVID questions
T. Rama Prasad https://www.thehindu.com/opinion/open-page/covid-questions/article65803119.ece
AUGUST 28, 2022 01:08 IST
UPDATED: AUGUST 27, 2022 14:16 IST
The pandemic has given rise to a breed of inquisitive patients who want to know all about the infection

A patient asked me whether she may have ‘Corbevax’ as a ‘booster’. I said: “Why not, it’s available in India since August 12, 2022.” Seemingly unconvinced by my answer, she said that the WHO had not approved it. She then wanted to know whether COVID vaccines would protect her. I said: “Why not, because of the vaccines we are now able to move about freely.” Came the answer: “But, doctor, the highly cautious American President Joe Biden, British Quee
n Elizabeth II, and the young U.S. Surgeon-General Dr. Vivek Murthy got the infection after multiple vaccinations.”
To convince the patient of the goodness of the vaccines, I explained: “Occasionally, ‘breakthrough’ infections may occur, but the disease won’t be severe.” She then queried if ‘Paxlovid’ may be taken in the case of such infections. Surprised by her knowledge on COVID treatment, I again said: “Why not, it must be beneficial.” Betraying a tinge of derision, she said that Biden had ‘Paxlovid rebound’ infection. I didn’t say it out loud, but this is the problem in handling ‘Internet-educated’ patients.
After all these questions, the patient wanted to know whether it is safe to take ‘Covishield’ and ‘Covaxin’. I said: “Why not, we gave them to most of our eligible population with a good safety profile.” With an expression of amusement, she pointed out that many countries stopped using ‘Covishield’ (Oxford AstraZeneca) for some time due to dangerous blood clots, and that the WHO had suspended supply of ‘Covaxin’ through United Nations agencies. Even before I started to explain, she said three Canadian doctors “had died after taking COVID vaccine, all within a week in July 2022”. With clinical coolness, I countered that the deaths were stated to be not related to vaccination. With a wry smile, she made a sarcastic comment: “Yes, yes, it was stated that the death of our comedian movie actor Vivek, one day after being vaccinated, was also not related to the vaccine.” I decided not to get into the quagmire of controversies.
She then wondered if the vaccine was so dangerous that Novak Djokovic preferred to forego the French Open and Wimbledon titles rather than getting vaccinated. I curtly said: “There are stupid people who opposed measles vaccine and let their children die. Brazilian President Jair Bolsonaro said that COVID vaccines would convert people into crocodiles. Former U.S. President Donald Trump touted hydroxychloroquine and wondered why disinfectants are not injected into people.” The patient reinforced her stance saying that some recent reports said that polio was spreading in rich countries through the ‘Oral Polio Vaccine’. I said I didn’t know anything about it.
She was curious to know whether ‘Remdesivir’ had any role in treatment. I said, “Why not, in a few cases it may be beneficial.” She commented that the drug was grossly overused to the tune of ₹593 crore from June to December 2020 in India where the need might have been only a fraction of that amount. She asked me whether taking medicines was safe at all. Defensively, I said: “Why not, millions of lives are saved every day.” She remarked that the risk of being harmed during medical treatment is one in 300, while it is one in 1,000,000 in air travel, and that 750 older adults are hospitalised every day due to side effects of medicines in America alone.
Then she went on to question about the validity of studies on COVID published in medical journals. Meekly, I said: “Because of the evidence-based publications, millions of lives could be saved, and life on Earth could become almost normal within three years after the onset of the pandemic. We should say hallelujah.” With a winning smile, she cited the infamous articles that were published and retracted in famous journals like The Lancet and The New England Journal of Medicine using allegedly fraudulent and fabricated data generated by the Surgisphere. I said: “Of course, that’s an aberration, black sheep are there in every field from paleontology to nanotechnology.” She took a dig at my profession, saying that modern medicine is getting a taste of its own medicine.
Then she wanted to know about the utility of “lockdowns”. I said, “Lockdowns contained the disastrous spread of COVID and prevented a lot of deaths.” Unconvinced, she asked: “Did not the lockdowns indirectly kill a lot more non-COVID patients and would not they continue to kill more in the future as a fallout of the economic downslide?”
Finally, she asked me why I had spent so much of my time talking to her. I said: “At the age of 80, I am not ‘young and ambitious’ to build up practice; now, I usually give appointments for only two patients a day.” All the while, she was doing the questioning and I’d been answering her patiently. Now, it was my turn to ask her: “What’s your medical problem, madam?”
She replied that she had come only to get to know something about COVID and inquired about the consultation fee to be paid. I said: “You are not a patient and I didn’t treat you. You need not pay anything. Even if you are my patient, this is the ‘Pay What You Can Clinic’.” She looked at me as if I were a fool kicking away a pot of gold, and then wanted to know more about the clinic, me and... COVID.
Dear Reader,
If you also want to know more about “the clinic, me and … COVID”, just as the “above patient”, please click on: https://drtramaprasad.blogspot.com/2017/04/dr-t-rama-prasad.html
T. Rama Prasad
There are only 10 faces in this drawing, but the COVID has many more !
The face of COVID would be remembered for a longer time than any of the faces in the ‘tree’ above. Of course, everybody would be forgotten in course of time. And the ‘time’ is a very relative thing. Just see the ‘timeline’ below:
'Age' of the Sun -- 4.54 billion years. Expected lifespan. -- 7 billion years more
'Age' of the Earth -- 4.54 billion years. Expected lifespan -- 1 billion years more
'Age' of Himalayas -- 50 million years
'Age' of Humans. -- 3 lakh years
'Age' of Religions -- 4 thousand years
'Age' of Temples. -- 3 thousand years
‘Age’ of viruses -- 3.5 billion years
‘Age’ of viral epidemics -- 12,000 years
‘Age’ of COVID – about 3 years as in 2022
We have around 380 trillion viruses (mostly harmless) on or inside our bodies !!!
“Computer Virus” is a “Mechanical Organism”, such as a computer code, which may damage computers, ‘copy’ itself and ‘infect’ other computers, just like a “Biological Virus.
Dr. T. Rama Prasad
A BLOG ARTICLE in : http://drtramaprasad.blogspot.com

A brief introduction
In the words of Prof C H Sivaraman, FRCP (London):
“ ... Dr. T. Rama Prasad belongs to a distinctly different and unconventional species of doctors. He speaks sparingly and does not even display his qualifications or merits, but his innumerable published writings (he calls them ‘scribblings’ though they are ‘pearls of wisdom and knowledge’, sprinkled with a bit of humour and sarcasm) which received wide acclaim talk eloquently for him. The ‘PAY WHAT YOU CAN’ Clinic where services are available for which one may pay whatever one can is a facility run by Dr. Prasad for a very long time which could be a world record. Dr. Prasad is called a “god” by his patients, and many of them named their children after his name “Prasad” -- that is the height of recognition of goodness of a human being.."
Service to Humanity is service to God; Kindness costs nothing
This is an odd lifetime study. A study to realise the reality. Most of the people love to be charitable, but few contribute. Read about GORU.
An anecdote about “GORU”
During my childhood, one of my schoolmates had huge nails. Her name was Gowri. We nicknamed her as ‘Goru’ (‘goru’ in Telugu means nail of a finger or toe ). They used to say that her huge nails caused a problem in her heart. It might be a case of ‘Digital Clubbing’ (abnormal nails present in some ‘Congenital Heart Diseases’). After one summer vacation, ‘Goru’ didn’t come back to the school. It was learnt that she died due to the nail / heart problem, and that treatment could not be availed as they didn’t have money to pay for it.
Perhaps, this incident prompted me to look at everyone’s nails from that time which might have led me to report the first case from India of ‘Yellow Nail Syndrome (YNS)’ in 1980 (published in an American journal, CHEST) and the first case in the worldof ‘Yellow nails & Covid’ in 2023, published in an Indian journal, THE ANTISEPTIC - https://drtramaprasad.blogspot.com/2017/04/yellow-nail syndrome_28.html
And perhaps, the preventable death of ‘Goru’ due to the inability to pay for the treatment motivated me to start my ‘PAY WHAT YOU CAN’ Clinic (PWYCC) half-a-century ago where patients may pay whatever they can. No fixed fee ( http://drtramaprasad.blogspot.com/2017/06/pay-what-you-can-clinic.html ). The credit for these case reports on YNS and the starting of my PWYCC should go to ‘Goru’. Thanks to “Goru”.
-- T. Rama Prasad

******************************************
Dr. T. Rama Prasad’s ‘PAY WHAT YOU CAN’ Clinic
“Thena thyakthena bhoojithaha”– Ishopanishad
( Translated by Prof. B.M. Hegde as: “Rejoice in giving.”)
True to this quote, I have been rejoicing at what little I could give. Defying stereotypes, this clinic has been in existence for a very long time, sans glitz, blitz, ads, microphones, speeches and noise. As a matter of my policy, publicity is shunned. The reason is simple. Good work needs no noise and nonsense. My ‘SCRIBBLINGS’ on related topics may be accessed at: http://drtramaprasad.blogspot.com

Yes, ‘PAY WHAT YOU CAN & WISH’, as consultation fee. It is the patient’s choice. It may even be zero. The patient may pay (donate) any amount. The money may just be put into the ‘hundi’ box, or remitted through the ‘Google Pay/UPI’ QR code / UPI number 9842720393 / UPI ID : drtramaprasad@okhdfcbank.
And the money thus received is used for charity to help the needy, the poor and the less fortunate.
If interested to know more about this facility, go to: http://drtramaprasad.blogspot.com/2017/06/pay-what-you-can-clinic.html .
And, even if you are not a patient, and if you wish, you may also 'contribute whatever you can' in the same way.
"We need not run after money. If we are meritorious and compassionate, money would run after us, and it eludes us if we run after it.” -- T. Rama Prasad
“Richness is not having lots of money. It is the feeling that one has enough of it. Contentment sans comparison is what makes one really rich.”
-- T. Rama Prasad.
Facebook: T Rama Prasad Twitter: @DrRamaprasadt Telegram : Dr T Rama Prasad

Consult your local doctor before rushing to me.
Most ailments can be cured at local level.
For APPOINTMENT with Dr. T. Rama Prasad, contact : 98427 20393
More at : https://drtramaprasad.blogspot.com/2017/04/dr-t-rama-prasad.html
********************************************************
Facebook: T Rama Prasad Twitter: @DrRamaprasadt Telegram : Dr T Rama Prasad
Consult your local doctor before rushing to me
Most ailments can be cured at local level
Dear Dr. Rama Prasad
I am sure the world will be a better place, if people understand your writings ... ‘EXCELLENT’ is the word. I cannot find any other word in this language to describe what you have written without any pretensions. You have brought out some home truths to those who care to read your website ... You are a great thinker, writer and crusader ... As usual, your messages are incisive, to the point and make lots of sense, much better than my articles …
... You are not only GREAT, but are a true missionary in medicine. May your tribe increase for the good of mankind. ….
Love,
-- Padma Bhushan Prof. B. M. Hegde, (awarded Padma Vibhushan in 2021)
MD, FRCP (Lond), FRCP (Edin), FRCP (Glas), FRCP (Dub), FACC (USA), FAMS, Former Professor of Cardiology, Middlesex Hospital Medical School, University of London, UK, Former Vice-Chancellor, Manipal University, India, Affiliate Professor of Human Health, Northern Colorado University, USA, Editor-in-Chief, The Journal of the Science of Healing Outcomes, Chairman, State Health Society’s Expert Committee, Govt of Bihar, India and Padma Bhushan awardee of 2010. www.bmhegde.com
CLICK ON THE HEADINGS BELOW TO ACCESS THE “SCRIBBLINGS”
MY LOVE STORY & good old days (4) BETTER HALF (4) SHIVA, KRISHNA, Ramanuja & Ramanujan (5) MOTHER-IN-LAW (6) YOU ARE NOT OLD (7) MODERN MEDICINE -- the Good, the Bad and th... (8) Dr. Peon, PhD (9) MEDICAL CONFERENCES & Clinical meetings (10) RUN ON MONEY (11) MEDICINE IN RURAL INDIA (12) RURAL ARE THE REAL (13) INTERNET EFFECT (14) MARKETING TRICKS & INNOVATIONS (15) INCREDIBLE INDIA ! (16) SCHOOL EDUCATION (17) DEVALUED DEGREES (18) TEA, COFFEE and COMMERCE (19) SEX. and MARRIAGE (20) THE CHANGING WORLD (21) RAPE (22) SEXUAL HARASSMENT (23) DRESS SENSE (24) OPEN AIR DEFECATION (25) ONAM 2017 (26) TEST-TUBE BABIES and TERMINATION BABIES (27) TEST-TUBE PUPPIES (28) ASTHMA, ALLERGY & COPD (29) GIRL CHILD : GOLDEN CHILD (30) MY REAL AWARDS (31) TREES and PLANTS (32) PERUNDURAI MEDICAL COLLEGE & SANATORIUM campus (33) SOPHISTICATED CHEATING (34) NIPAH & ZIKA viruses (35) SWINE FLU -- A (H1 N1) influenza (36) INDIAN SUPERBUG (37) HCQ, IVERMECTIN, CORONAVIRUS and FRAUDS (38) YOGA (39) CORONA and CHARLES DARWIN (40) GOD, RELIGION & UNIVERSE (41) LOCKDOWN MEDICINE (42) CODUP (43) GOD-MEN (44) DOGS (45) CANCER (46) SMILE and STRESS (47) CIVIC SENSE & MANNERS (48) MY ART (49) TUBERCULOSIS in India (50) DIABETES (51) FOOLED TO BELIEVE (52) DENGUE, ZIKA and MOSQUITO (53) COMPLEXION (54) BAHUBALI (55) VINAYAKA chathurdhi 2017 (56) SUNDAY LUNCH ... Dec 3, 2017 (57) ABDUL KALAM (58) BIRDS and DRUGS (59) YELLOW NAIL SYNDROME (60) RICHNESS and HAPPINESS (61) FISHES (62) KMCH (63) MY 'SCRIBBLES' IN NEWSPAPERS (64) To live in INDIA or ABROAD ? (65) SILENT, ISOLATED and INSULATED (66) PONGAL FESTIVAL (67) SPB (68) CESAREAN DELIVERY (69) POLLUTION, Disease and Deepaavali (70) HAPPY 2018 (71) BRINGING UP CHILDREN (72) SINGAPORE (73) STAFF & STUDENTS. -- photos (74) "AHIMSA" (75) GRADUATION DAY -- 2018, Perundurai Medical Col... (76) PERUNDURAI is the GEM (77) WORLD CANCER DAY ..February 4, 2017 (78) INDIAN ENGLISH (79) FOOD, EXERCISE and SLEEP (80) Nurses Day 2017 (81) DEEPAAVALI (82) PUTHAANDU -- Tamil New Year Day - 2018 & 2017 (83) COMPUTER. ILLITERATE (84) SMILE and LAUGHTER (85) REMOTE ANCESTORS (86) ODD things ... wow, whacky & weird ! (87) FACEBOOK 'scribbles' (88) HANDWRITING (89) MY QUOTES
GREAT HOLY SOUL
16.10.2017
" ... I always wonder that we both seem to be identical in our thoughts, deeds and actions. ... I always cherish your friendship and appreciate your humanitarian attitude towards life, poor rural people and the needy. ... I went through your articles ... especially, the 'PAY WHAT YOU CAN Clinic' touched my heart, and after studying, I wondered: "What a great holy soul you are !" You are a living example of Swami Vivekananda. ... "
Dr. J.K.K. Munirajahh, M.Tech (Bolton)
Chairman, JKKM Group of Institutions & Industries
Komarapalayam, Tamil Nadu, India
----------------------------------------------------
"...A study of your work reveals how fertile is your brain and how facile is your pen. Your command of English is breathtaking. One cannot help being astounded by your encyclopaedic range of knowledge and its depth is unfathomable......Your sense of humour is very much to be appreciated. Your invaluable treasure "SCRIBBLINGS" is to be preserved for posterity....."
05.08.1999 -- Prof. P. Lakshmi, MA,
Principal, Vellalar College for Women,
Thindal, Erode, Tamil Nadu, India
Dear Dr. Rama Prasad, 20 Jan 1999
--------------------------------------------------
“..When I saw a copy (of your book titled "Some of my SCRIBBLINGS") in the medical college library, curiosity got the better of me and I borrowed it. As I went through it, curiosity turned into admiration. What struck me first and the most was your command over the language. I appreciated your interest in widely varied subjects, from pornography to piano, as the saying goes. I also realised that the interest was not just superficial, but substantial as evidenced by the statistics quoted to emphasise a point. When I finished with it, it left me wondering how you continued to sustain your interest despite having spent more than 3 decades in this place, well isolated and insulated from academic and intellectual environment...”
--- Group Captain (Retd) Prof. N. Ramachandran, MD,
Professor of Paediatrics, Perundurai Medical College Perundurai, Erode District, Tamil Nadu, India
---------------------------------------------
“… I am amazed to find how the book (Some of my “Scribblings”) mirrors your multifaceted personality – the sterling qualities of head and heart. It reflects the encyclopaedic range of your mind. I am struck by the fact that there was no subject that is untouched – from physical to metaphysical, sacred to secular, all under the sun have been dealt with quite thoroughly, authenticated and well-documented to reveal a genuine humanist at work. … Combined with the art of healing is your art of drawing and painting. … We are amazed to see your paintings and to learn that the illustrations in the “Scribblings” are your own. …”
-- Prof. V. Prafulla,
M.A., Ph.D. (Eng.), M.A. (Hindi), P.G.T.E., Former Principal, Erode Arts College for Women, Erode, Tamil Nadu, India; Former Professor of English, Visalakshi College, Udamalpet, Tamil Nadu, India.
April 12, 2020

The following is the comment written by the internationally renowned scholar, Pritam Bhattacharyya (Editor-at-Large of Pentasect and Founder and Chief of Wordsmith at Wordsmith Communication, Chairman of Freelance Foundation, ) on the blog article on Coronavirus and COVID-19
(1) https://wordsmithofbengal.wordpress.com/2012/01/16/health-un-heath-and-fear-of-un-health/
(2) https://wordsmithofbengal.wordpress.com/2012/04/23/google-effect-and-kali-yuga-prophecies/
wordsmithApril 12, 2020 at 10:42 PM
“One of the best articles I have read on this theme and having balance, measure and proportion. Miss Corona in hindsight is really kind and benign in a sense - Nature has rolled a dice with fatality of 2-3%. She is under no obligation not to roll a dice of fatality 40,50,60% with Ms. Corona being "size zero" and "air-borne". Consider what would have happened ?
Dr. Prasad is one of the few doctors whom I know who fall into the rare category of "healers". A healer knows the art, science and commerce of healing, i.e. allowing the innate immunity of the body to manifest itself.
One should be very careful and critical about three things in the world : Big Pharma, Big Government, Big Science. In the proverbial Kali-Yuga, all three converge with overlapped agendas and sometimes not with the best interest in mind of the end users : patients, citizens, learners.
Finally, this pandemic will also pass. The system will come to a new equilibrium. But I think a whole generation will carry this impression forward and may become saner with this.
I nurture another hope : just like pivotal events propel a whole generation (Apollo Mission and interest in space science), this may inspire many young Indians to shift their focus into public healthcare, virology, immunology, public immunity, psychological counselling and learning the art and science of healing.
Again, it was very nice to find an article of this time in the avalanche of printed words in this theme.
Continue your good work.”
‘COVID Medical Literature – the Good, the Bad and the Ugly’ The Antiseptic, September 2022, Vol 119, No 9
From the Editor........
The Editor wishes to advise the readers of ‘The Antiseptic’ who are interested in having correct, complete and comprehensive knowledge of the current literature on Covid, to read the above article by Dr. T. Rama Prasad, written as is usual, in beautiful, flawless and inimitable English, with numerous apt quotations.
He further wishes to thank Dr. T. Rama Prasad profusely for choosing to publish all his ‘very interesting to read’ articles on Covid in ‘The Antiseptic’ and hopes that he (Dr. T. Rama Prasad) continues his benevolence.
-----------------------------------------------
I am greatly honoured and recognised, indeed, by this special ‘editorial comment’ of inspiring appreciation by the distinguished, scholarly, erudite, and eclectic editor of the premier journal, The Antiseptic, which itself is a rare treasure of documentation from the eclecticism of India’s diverse medical systems, including the dominant ‘modern medicine’. My articles were published in this long-standing and reputed journal even more than forty years ago.
-- T. Rama Prasad


COVID world: 24 of my articles on ‘COVID’ were published in 24 months in Medical Journals which is a WORLD RECORD in Medical Journalism.
This article titled “Origin of COVID” is the 24th one.
-- Dr. T. Rama Prasad, ‘PAY WHAT YOU CAN’ Clinic, Perundurai, India
---------------------------------------------------------------------------------------------
. Origin of COVID .
RAMA PRASAD T.
Dr. T. Rama Prasad,
Formerly: Medical Superintendent (Special) of RTS & IRT Perundurai Medical College and Research Centre,
Perundurai, Tamil Nadu, India.
Presently: Director of ‘PAY WHAT YOU CAN’ Clinic, Perundurai, Erode District, TN – 638052. drtramaprasad@gmail.com WhatsApp +91 98427 20393 BLOG https://drtramaprasad.blogspot.com
WEBSITE www.rama-scribbles.in Twitter @DrRamaprasadt Facebook T Rama Prasad
Telegram Dr T Rama Prasad
`
A MONTHLY JOURNAL OF MEDICINE AND SURGERYSN
Vol. 119 No. 8 August 2022 ISSN 0003 599
Indexed in IndMED Email: admin@theantiseptic.in www.theantiseptic.in
Some COVID
articles authored by
Dr. T. Rama Prasad
and published in MEDICAL JOURNALS, making a WORLD RECORD
Rama Prasad. T., Origin of COVID. The Antiseptic, 2022 August; Vol. 119; No. 8; P: 09-17; Indexed in IndMED – www.antiseptic.in
Rama Prasad. T., COVID Deaths. The Antiseptic, 2022 July; Vol. 119; No. 7; P: 14-22; Indexed in IndMED – www.antiseptic.in
Rama Prasad. T., The long and the short of COVID in India. The Antiseptic, 2022 June; Vol. 119; No. 6; P: 14-27; Indexed in IndMED – www.antiseptic.in
Rama Prasad. T., COVID Fear and Paranoia. The Antiseptic, 2022 May; Vol. 119; No. 5; P: 09-17; Indexed in IndMED – www.antiseptic.in
Rama Prasad, T., Post-OMICRON Peregrination. The Antiseptic, 2022 April; Vol. 119; No. 4;
P: 06-14; Indexed in IndMED – www.antiseptic.in
Rama Prasad, T., COVID – still an enigma. The Antiseptic, 2022 March; Vol. 119; No. 3; P: 20-25; Indexed in IndMED -- www.antiseptic.in
Rama Prasad, T., OMICRON – A Paper Tiger. The Antiseptic, 2022 February; Vol. 119; No. 2; P:12-21; Indexed in IndMED – www.antiseptic.in
Rama Prasad, T., Ominous Omicron of COVID. The Antiseptic, 2022 January; Vol. 119; No. 1;
P:25 – 29; Indexed in IndMED – www.antiseptic.in
Rama Prasad, T., COVID and Tuberculosis. The Antiseptic, 2021 December; Vol. 118; No.12;
P: 11-17; Indexed in IndMED -- www.antiseptic.in
Rama Prasad, T. The Science and Nonsense around COVID. The Antiseptic, 2021 November; Vol. 118; No. 11; P: 8-14; Indexed in IndMED -- www.antiseptic.in
Rama Prasad, T. COVID, Children and Schools. The Antiseptic. 2021 October; Vol.118; No.10; P: 08-18; Indexed in IndMED -- www.antiseptic.in
Rama Prasad, T. India’s Third COVID Wave. The Antiseptic. 2021 September; Vol.118;
No.9; P: 14-20; Indexed in IndMED – www.antiseptic.in
Rama Prasad, T. Vagaries of India’s COVID Vaccination Policy. The Antiseptic. 2021 August; Vol.118; No.8; P: 10-16; Indexed in IndMED – www.antiseptic.in
Rama Prasad, T. Mucormycosis and COVID-19 in India. The Antiseptic. 2021 July; Vol.118; No.7; P: 21-26; Indexed in IndMED -- www.antiseptic.in
Rama Prasad, T. Disastrous Second COVID Wave in India. The Antiseptic. 2021 June; Vol.118; No.6; P: 20-27; Indexed in IndMED – www.antiseptic.in
Rama Prasad, T. COVID Variants. The Antiseptic. 2021 May; Vol.118; No.5; P: 11-14; Indexed in IndMED -- www.theantiseptic.in
Rama Prasad, T. Covishield or Covaxin ? The Antiseptic. 2021 April; Vol. 118; No. 4; P: 12-16; Indexed in IndMED – www.theantiseptic.in
Rama Prasad, T., Versha Rajeev. The Conundrum of COVID-19 Vaccines. The Antiseptic. 2021 January; Vol.118; No.1; P: 10-17; Indexed in IndMED – www.theantiseptic.in
Rama Prasad, T. 40+15 Hypoxia Test in COVID-19. The Antiseptic. 2020 December; Vol. 117; No. 12; P: 13-17; Indexed in IndMED – www.antiseptic.in
Rama Prasad, T., Versha Rajeev. Antiseptics, Disinfectants and COVID-19. The Antiseptic. 2020 November; Vol.117; No.11; P: 26-28; Indexed in IndMED – www.antiseptic.in
Versha Rajeev., Rama Prasad, T. Fear and COVID. Health. 2020 November; Vol.98; No.11; P:31-32
Rama Prasad, T., Versha Rajeev. Tea and COVID. Health. 2020 October; Vol.98; No.10; P: 4-6.
Rama Prasad, T. Is the “Lockdown Medicine” too toxic ? The Antiseptic. 2020 October; Vol. 117; No. 10; P: 13-15; Indexed in IndMED – www.theantiseptic.in
The articles may be accessed at IndMED – www.antiseptic.in
WRITINGS AND TALKS of Dr. T. Rama Prasad
List No. 1
1. Drug Resistance in Tuberculosis - Journal of the Indian Medical Association, Vol. 64, pp. 264-267, 1975.
2. Digital clubbing and Hypertrophic Pulmonary Osteoarthropathy - Pathogenesis - The Antiseptic, Vol. 76. pp.
213- 215, 1979.
3. Childhood Tuberculosis - Part I - The Antiseptic, Vol. 76, pp. 449-504,1979
4. Childhood Tuberculosis - Part II - The Antiseptic, Vol. 76. pp. 567-574, 1979
5. Yellow Nail Syndrome - Chest (U.S.A.), Vol. 77, p.580, 1980 –
http://journal.chestnet.org/article/S0012-3692(16)40458- 7/fulltext
6. Short-course Chemotherapy - The recent Advances in the Treatment of Respiratory Tuberculosis - Current Medical Practice,
Vol.24, pp. 41- 46, 1980.
7. Stevens-Johnson Syndrome and Thioacetazone - The Antiseptic, Vol. 77, pp. 99-102, 1980.
8. Yellow Nail Syndrome - The Indian Journal of Chest Diseases & Allied Sciences, Vol. 22, pp. 69-72, 1980.
9. Highly Purified Insulins - An Assessment - The Antiseptic, Vol. 77, pp. 3455-347, 1980.
10. Diabetes and Tuberculosis - The Medicine and Surgery, Vol. 21, pp. 10-12, 1981.
11. Tuberculosis Control in India - In Press
12. Tuberculin Test - Relevance to diagnosis in India today - In Press
13. Toxic Epidermal Necrolysis - The Antiseptic, Vol. 75, p. 194, 1978.
14. Drugs in the treatment of Tuberculosis - The Antiseptic, Vol. 75, p.678, 1978
15. Chemotherapy of Tuberculosis - The Antiseptic, Vol. 76, p.248, 1979.
16. Streptomycin in Tuberculosis - The Antiseptic, Vol. 76, p.516, 1979.
17. Health of the citizen (Special article) - The Hindu, Vol.99 A, No.198, p.8, 1976
18. How effective is the TB control programme ? (Special Article) - The Hindu, Vol.100, No. 274, p.8, 1977.
19. Five years Plans and TB Control Programme (Special Article) - The Hindu, Vol.101, No. 275,
20. BCG vaccination - The Antiseptic, Vol. 76, p. 726, 1979.
21. Genetic Selection - The Antiseptic, Vol. 77, p.258, 1980.
22. National Tuberculosis Control Programme - views presented, on invitation by the Tuberculosis Association of India,
at the 32nd National Conference on Tuberculosis and Chest Diseases, 1977.
23. Correlation between Geomagnetic Activity and Haemoptysis - paper presented at the II Tamil Nadu State Conference
on Tuberculosis & Chest Diseases, 1980.
24. Snakes.
25. AIDS - the disease of the decade - Radio Talk - All India Radio, Coimbatore, Feb. 1, 1986.
26. AIDS - What next ? - Radio Talk - All India Radio, Coimbatore, May 24, 1986
27. BRAIN FEVER (Encephalitis): taming the scourge - Radio Talk - All India Radio, Coimbatore, February 14, 1987.
28. HEALTH OF THE HIGH RISK GROUPS: Mothers, Children and elderly - Innovative Health Care Programmes,
Paper submitted for Scientific Session of the National Annual Conference of the Indian Society of Health administrators.
29. SAVING THE YOUNG - healthcare of the children in developing countries - Radio Talk -
All India Radio, Coimbatore, January, 1988.
30. MEDICINE and MONEY - Co-Chamber Journal, Vol. 5, Issue 8, p.8, 2010,
31. THE INDIAN SUPERBUG - Co-Chamber Journal, Vol. 5, Issue 9, p.15, 2010
32. SWINE FLU - Co-Chamber Journal, Vol. 5, Issue 10, p. 13
33. HEALTH CHECK-UP: how healthy is it ? - The Hindu, Open Page, Jan. 15, 2012 -
……http://www.thehindu.com/opinion/open page/article2801701.ece
34. THE ‘GOOGLE EFFECT’: may be good, may be bad - The Hindu, Open Page, April 22, 2012
...http://www.thehindu.com/opinion/open-page/article3340116.ece
35. OF TEA, COFFEE and COMMERCE - The Hindu, Open Page, January 12, 2014 …
… http://www.thehindu.com/opinion/openpage/of-tea-coffee-and-commerce/article5567951.ece.
36. A BAD PATCH - The Hindu, OPEN PAGE, March 15, 2020 ...
https://www.thehindu.com/opinion/open-page/a-bad-patch/article31069356.ece
37. MODERN MEDICINE: how good is it in India ? - Co-Chamber Journal, Vol. 11, Issue 5, p. 23, June 2016 & Vol. 11,
Issue 6, p. 18, July 2016
38. WORLD TB DAY: March 24, 2016 - Health, Vol. 94, No. 5, p. 20, May 2016
39. IS THE "LOCKDOWN MEDICINE" TOO TOXIC ? -- The Antiseptic, Vol.117, No.10, pp. 13 -15, 2020
40. ANTISEPTICS, DISINFECTANTS and COVID-19 -- The Antiseptic, Vol.117, No.11, pp. 26 - 28, 2020
41. 40+15 HYPOXIA TEST in COVID-19 -- The Antiseptic, Vol.117, No.12, pp.13 –17, 2020
42. THE CONUNDRUM of COVID-19 VACCINES – The Antiseptic, Vol. 118, No. 1, 2021
43. Fear and COVID-19 – HEALTH, Vol. 98, No. 11, pp. 13 -14, 2020
44. Tea and COVID-19 – HEALTH, Vol. 98, No. 10, pp. 4 – 6, 2020
List No. 2 contains references to about 1000 writings which may be found on my Website -- T. Rama Prasad
“Education is the most powerful weapon we can use to change the world.” --- Nelson Mandela
AUTHOR Dr. T. Rama Prasad
A short list of some of the published articles in The Antiseptic (a premier Medical & surgical journal),
‘The Hindu’ (a national Newspaper), etc. authored by Dr. T. Rama Prasad.
1. Digital clubbing and Hypertrophic Pulmonary Osteoarthropathy -
Pathogenesis -- The Antiseptic, Vol. 76. pp. 213-215, 1979
2. Childhood Tuberculosis - Part I -- The Antiseptic, Vol. 76, pp. 449-504,1979
3. Childhood Tuberculosis - Part II -- The Antiseptic, Vol. 76. pp. 567-574, 1979
4. Stevens-Johnson Syndrome and Thioacetazone -- The Antiseptic, Vol. 77, pp. 99-102, 1980
5. Highly Purified Insulins - An Assessment -- The Antiseptic, Vol. 77, pp. 3455-347, 1980
6. Is the "Lockdown Medicine" too toxic ? -- The Antiseptic, Vol.117, No.10, pp. 13 - 15, 2020
7. Antiseptics, Disinfectants and COVID-19 -- The Antiseptic, Vol.117, No.11, pp. 26 - 28, 2020
8. Disastrous Second Covid Wave in India -- The Antiseptic, Vol.118, No. 6, pp. 20-27, 2021
9. Covid Variants -- The Antiseptic, Vol. 118, No.5, pp. 11-14, 2021
10. The Conundrum of COVID-19 Vaccines -- The Antiseptic, Vol.118, No. 1, pp. 10-17, 2021
11. Covishield or Covaxin ? -- The Antiseptic, Vol.118, No. 4, pp. 12-16, 2021
12. 40+15 Hypoxia Test in COVID-19 -- The Antiseptic, Vol. 117, No.12, pp. 13-17, 2020
13. Mucormycosis and COVID-19 in India -- The Antiseptic, Vol. 118, No. 7, pp. 21-26, 2021
14. Vagaries of India’s Covid Vaccination Policy – The Antiseptic, Vol. 118, No. 8, pp. 10-16, 2021
15. India’s Third Covid Wave -- The Antiseptic, Vol. 118, No. 9, pp. 14-20, 2021
16. Covid, Children and Schools -- The Antiseptic, Vol. 118, No. 10, pp. 08-18, 2021
17. The Science and Nonsense around COVID -- The Antiseptic, Vol.118, No.11, pp. 08-14, 2021
18. Covid and Tuberculosis – The Antiseptic, Vol.118, No.12, 2021
19. Tea and Covid -- Health, Vol. 98, No.10, pp. 4-6, 2021
20. Fear and Covid -- Health, Vol. 98, No. 11, pp. 31-32
21. HEALTH CHECK-UP: how healthy is it ? - The Hindu, Open Page, January 15, 2012 –
https://www.thehindu.com/opinion/open-page/Health-check-up-how-healthy-is-it/article13379235.ece
22. THE ‘GOOGLE EFFECT’: may be good, may be bad - The Hindu, Open Page, April 22, 2012
23. OF TEA, COFFEE and COMMERCE - The Hindu, Open Page, January 12, 2014 …
https://www.thehindu.com/opinion/open-page/of-tea-coffee-and-commerce/article5567951.ece
24. A BAD PATCH - The Hindu, Open Page, March 15, 2020 ...
https://www.thehindu.com/opinion/open-page/a-bad-patch/article31069356.ece
25. Yellow Nail Syndrome - Chest (U.S.A.), Vol. 77, p.580, 1980
https://journal.chestnet.org/article/S0012-3692(16)40458-7/fulltext
26. Yellow Nail Syndrome - The Indian Journal of Chest Diseases & Allied Sciences, Vol. 22, pp. 69-72, 1980.
27. Drug Resistance in Tuberculosis - Journal of the Indian Medical Association, Vol. 64, pp. 264-267, 1975.
References to more articles by Dr. T. Rama Prasad may be found in: http://drtramaprasad.blogspot.com

Dr. T. Rama Prasad www.rama-scribbles.in
LOVABLE RURAL FOLK ... February 10, 2018
Yes, rural are really lovable folk. Most of them have a refreshingly rural and innocent background. They have blind faith in gods, and doctors as well.
After a few decades, we may see no more of such good plain-hearted rural folk. And, even now, we rarely see the good old grand grandmother of ‘topless’ (‘blouseless’) era ! The women of that generation cover their upper bodies with a piece of a cloth only (end piece of saree) wrapped around without any underclothing like bra or blouse.
Today (February 10, 2018), one frail-looking grandmother in that 'topless' attire (see the attached photo) walked into my consultation chamber, accompanied by her grandson, but not needed to be assisted by him to walk in. She (Gowandayamml) fluently talked in the grand old style ... said she got the appointment with great difficulty (limited consultations today, as I had to spare some time to attend my granddaughter's 'food court bonanza' at her school). At the end of the consultation, she wanted a 'cough syrup' (most of the 'cough syrups' are used unnecessarily and for psychological satisfaction, and to the great delightfulness of drug industry !). I gave her a sample bottle of a cough syrup, free of cost, of course ... and lo and behold, her face was lit up with happiness. Little pleasures ... little things matter in life ... read the 'Scribbling' titled 'Richness & Happiness' on my blog. She narrated at length of her previous visits over decades and profusely thanked me for keeping her fit (in fact, it is her good old lifestyle and her constitution that kept her fit, not me !). I asked her whether I may have a photo with her. She was amused and laughed. I called the receptionist to take a photo. The lady of the old school put up a serious pose for the photo. Receptionist, Nandhini, asked her to smile ... in vain ... perhaps, the grandma thought that one should not move or smile when the camera clicks (In our school days, photographers used to instruct us not to move or smile when they take group photos in the school, with those bulky 'plate' cameras with a long exposure time !). I shall give her a print of the photo when she visits me again ... curiously, we both are of the same age group by the calendar, though seem not to be by the images ! Finally, the plain, simple, candid and 'topless' granny left my chamber. After a while, she came back with money (hundred rupees notes) in her hand to put into my tiny 'Pay what you can' hundi, as consultation fee. I had to persuade her a lot not to give any consultation fee, saying that it's a great pleasure for me to treat her free of cost ... again there was a flash of a cheerful smile across her face. This is the most pleasant reward we get in medical practice -- the cheerful smile of satisfaction.
If you wish to read more about the good rural folk, click on http://drtramaprasad.blogspot.in/2017/08/rural-are-real.html
Reprinted from FACEBOOK … go to Facebook to read comments on this.
Dr. T. Rama Prasad, www.rama-scribbles.in http://drtramaprasad.blogspot.in
'PAY WHAT YOU CAN’ Clinic, Perundurai, Erode Dt., TN, India., Former Medical Superintendent (Special), RTS & IRT Perundurai Medical College and Research Centre, Perundura

WORLD HEART DAY … September 29
Various writings and ads (with commercial colour of discounts) appeared today across the globe scaring the public about their heart health. Some of them, purported to be of educative value to the public, may have a hidden agenda of vested interests. And, some normal persons may be converted into patients ! People are confused on knowing about needless tests, medicines and even surgeries.
Much of the modern treatment may be like cutting some of the branches of an evil tree without tackling the roots. ‘Modernity’ in lifestyle brought in its wake all the adverse factors, STRESS & ECOLOGICAL IMBALANCE (destruction of Nature) being the important ones, associated with money, materialism, competition, comparison, ego, hubris, hegemony, selfishness, greed, arrogance, anger, miserliness, manipulability, vanity, vengeance, etc. MODERNITY may be the root cause for the arrival of COVID. Moderns may have to mend their ways to prevent emergence of more novel viruses. Should we celebrate March 11 (March 11, 2020 was the day on which the WHO declared ‘Covid’ as a pandemic) as the ‘WORLD COVID DAY’ ? Or, should it be December 31 when the first outbreak in the world was reported in China in 2019 ?
Cell phones arrived, we forgot writing letters;
Automobiles arrived, we forgot walking;
Computers arrived, we forgot spellings;
Calculators arrived, we forgot mathematics;
Modern jobs arrived, we forgot families;
TVs arrived, we forgot cinema theatres;
Digital games arrived, we forgot playgrounds;
Modern pharma arrived, we forgot grannies’ remedies;
Speciality hospitals arrived, we forgot ‘MBBS clinics’;
Super-specialists arrived, we forgot family doctors;
Nuclear families arrived, we forgot relationships;
Junk food arrived, we forgot healthy meals;
Food courts arrived, we forgot cooking;
HEART specialists arrived, we forgot HEARTY meals !
COVID has arrived, we forgot everything else !
(I too forgot everything else, and authored 28 articles in 30 months, on only COVID, which were published in a single medical journal, The Antiseptic -- a WORLD RECORD in medical journalism !!!)
Dr. T. Rama Prasad,
https://drtramaprasad.blogspot.com www.rama-scribbles.in
drtramaprasad@gmail.com, Director, 'PAY WHAT YOU CAN' Clinic, Perundurai, Erode Dt., TN, India., Former Medical Superintendent (Special), RTS & IRT Perundurai Medical College and Research Centre.






The first outbreak of COVID in the world was reported in China on the very next day (31.12.2019) of taking the above photo on 30.12.2019 !!!
“We are sometimes praised and sometimes pilloried. We should neither bask in the glory of success nor sulk in the shadows of defeat.”



{kind=link}
The following is a list of some of my 'scribblings', including a few from the 28 articles on COVID published in a monthly medical journal in 30 months (a world record). To open them, click on any of the titles. -- T. Rama Prasad
Blog Archive
ReplyDeleteI’ve been living with Parkinson’s disease for some time, and nothing I tried seemed to make a lasting difference—until I began the herbal treatment from NaturePath Herbal Clinic. I was skeptical at first, but after about four months, I started to notice real improvements. My tremors became less frequent, my stiffness reduced, and my balance and coordination gradually began to improve.
For the first time in years, I feel more in control of my body and daily life. I can move more freely, sleep better, and even enjoy simple activities again without constant discomfort. The changes have been truly uplifting—both physically and emotionally.
If you're exploring natural options for managing Parkinson’s, I genuinely recommend giving this a try. It’s been a life-changing experience for me.
Learn more at: www.naturepathherbalclinic.com